CT and MRI are vital for the initial assessment and follow-up of acute thoracic injuries in professional rugby players and can have a decisive impact on patient management, an international team of researchers reported at RSNA 2012, during which attention also focused on sports injuries to the hand.
"Subtle injuries (in rugby players) may be missed on conventional radiography," noted lead author Dr. Daichi Hayashi, PhD, research assistant professor of radiology at Boston University School of Medicine. "Multimodality imaging including MRI and CT play an important role in the diagnostic process. Cross-sectional imaging helps in the decision-making process concerning return to training and competitive sport."
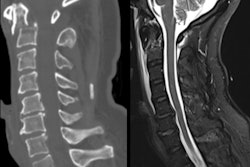
 A 26-year-old rugby player with a left-sided thoracic injury. Oblique coronal MR image (short tau inversion-recovery sequence) shows a chondral fracture of the eighth rib. Yellow arrow points to the site of fracture, where a small amount of fluid accumulation is depicted as hyperintensity. Image courtesy of Dr. Daichi Hayashi, PhD.
A 26-year-old rugby player with a left-sided thoracic injury. Oblique coronal MR image (short tau inversion-recovery sequence) shows a chondral fracture of the eighth rib. Yellow arrow points to the site of fracture, where a small amount of fluid accumulation is depicted as hyperintensity. Image courtesy of Dr. Daichi Hayashi, PhD.Traumatic thoracic injuries in rugby players are much less common than lower limb injuries, but the players are relatively more prone to such injuries due to the minimal protective wear compared to other contact sports such as American football, in which players wear protective clothing and helmets, he explained in an award-winning e-poster on this topic at the Chicago congress.
Rib injuries among rugby players tend to be most common in the fifth and ninth ribs, and they are often missed with conventional radiography and ultrasound. Always perform a CT scan with a multiplanar reconstruction (MPR) and volume-rendering technique (VRT), and use both CT and MRI for the acute stage, recommends Hayashi and his co-authors from the department of radiology at Klinikum Augsburg, Germany, the Australian Sports Commission, and Drs. Van Wageningen & Partners, Somerset West, South Africa. It is also necessary to consider nuclear medicine imaging for the delayed stage.
For an MRI examination of a suspected rib injury, the patient should be in a prone position, a marker should be placed, and axial and oblique coronal STIR (short TI inversion recovery) sequences should be obtained. T1-weighted sequences are not useful, and artifacts can be expected due to pulsation and breathing, they stated.
Other injuries that can be sustained during rugby matches occur in the thoracic spine, most likely secondary to a blow to the back or fall on the back. In rare cases, internal organs may be injured, but these are secondary to sternal/rib injuries. Cardiac contusion/tamponade and pneumothorax/hemothorax may also occur.
According to the injury surveillance study of the 2007 Rugby World Cup, there were 48 matches in seven weeks, constituting 1,920 player hours (1,024 for forwards, 896 for backs). Match injuries to the upper back/sternum/ribs occurred in 8.3/1000 player hours, while the comparable figure for the lower limbs was 45.8/1000 player hours. Thoracic injuries were more common in forwards (10.7/1000 player hours) than backs (5.6/1000 player hours), but when sustained, injuries were more severe in the latter group. A total of 12.4 days were lost from matches among the backs, against 5.8 days in the forwards.
Among the types of trunk injuries -- including the chest, abdomen, and back -- some were bone-related (14.6% of cases), while other injuries involved nonosseous joint structure/ligament (33.1%), muscle/tendon (43.1%), and others (9.2%).
In a four-season prospective cohort study that was published last year and featured 14 English premiership clubs and 899 players, the risk of absence due to chest injuries was higher in players whose position was full-back compared with other backs (Brooks JH, Kemp SP, British Journal of Sports Medicine, August 2011, Vol. 45, pp. 765-775). This was due to costochondral/sternal injuries, which led to 51 days' absence/1,000 hours, and the risk ratio (RR) to other backs was 2.27. Also in full-backs, rib fracture/contusion accounted for 36 days absence/1,000 hours, and the RR was 1.93.
Additionally, the risk of absence due to chest injuries was higher in loose-head props compared with other forwards. This was because of rib fracture/contusion (50 days absence/1,000 hours, RR = 3.51) and pneumthorax (25 days absence/1,000 hours, RR = 16.98).
 Injuries to skiers are common when the thumb gets caught in the ski pole during a fall.
Injuries to skiers are common when the thumb gets caught in the ski pole during a fall.
Another award-winning RSNA e-poster was dedicated to sports injuries to the hand, which are common in athletes. The return to activity requires prompt diagnosis and accurate treatment, and in general, ultrasound is fast and accurate, and allows dynamic assessment to assist in triaging patients into conservative and surgical management categories, according to lead author Dr. Roberta Dionello, from the Nuffield Orthopedic Centre in Oxford, U.K.
The ulnar collateral ligament (UCL) is an important stabilizer of the thumb, limiting radial abduction, particularly during a forceful grip or a pinch. The UCL lies deep to the adductor pollicis aponeurosis.
"Forced radial abduction of the thumb usually leads to tearing of the distal UCL. It is commonly seen in the acute setting in skiers whose thumb is caught in the ski pole during a fall," Dionello noted, whose imaging tips for skier's thumb include the use of a high-frequency transducer, use of a small footprint (or hockey stick) transducer, use of dynamic imaging, use of a thick jelly layer adjacent to bony prominences, and to compare sides.
"It can be difficult to identify the adductor aponeurosis in the static position. Use dynamic imaging with flexion and extension of the interphalangeal joint to move the aponeurosis, which is seen as a thin hypoechoic band gliding over the UCL," she added. "Image longitudinally along the ulnar aspect of the metacarpophalangeal joint (MCPJ) during flexion of the interphalangeal joint to determine whether the torn UCL is undisplaced, remaining deep to the aponeurosis (conservative) or the aponeurosis clashes against a displaced UCL (surgical)."
Acute annular pulley tears are commonly seen in rock climbers, who may suspend their whole body weight on flexed fingers. The most commonly injured digits are the ring and middle fingers, while the pulleys most often injured are those overlying the phalangeal shafts (A2 and A4), rather than the pulleys over the metacarpal and phalangeal heads, explained Dionello, whose co-author was Dr. Catherine McCarthy, also from the Nuffield Centre in Oxford.
The key finding on longitudinal views is bowstringing and volvar subluxation of the flexor tendon away from the phalangeal cortex, as in the case of A2 and A4 pulley tears, resulting in increased tendon-to-bone distance. Normal tendon-to-bone distance is less than 1 mm, fluid is often present in the posterior tendon sheath.
"The ruptured pulley can be identified based on the site of the maximal volar bowstringing. In A2 pulley tears, maximal volar displacement occurs over the proximal phalanx. In A4 pulley tears, maximal volar displacement occurs over the middle phalanx," the authors pointed out. "Scanning during forced flexion by pushing against the patient's finger tip enhances volar tendon subluxation, increasing diagnostic certainty."
In suspected cases of climber's finger, image longitudinally over the proximal phalanx and the metacarpal head, looking for increased bone-to-tendon distance enhanced by forced finger flexion, they recommend.
During flexion and extension of the fingers, the extensor hoods (or sagittal bands) retain the extensor tendons in the midline axis of the dorsal MCPJ, and this can lead to boxer's knuckle, according to Dionello and McCarthy. Chronic trauma to the metacarpal heads, typically seen in boxers, leads to injury of these structures. The extensor tendon is no longer held in place and subluxes with flexion.
"Image transversely over the metacarpal head and look for subluxation of the extensor tendon on finger flexion," they advise.
Finally, baseball or cricket player's finger encompasses two dorsal finger injuries that are often as a result of forced extreme flexion at the distal interphalangeal joint (DIPJ). Testing against resistance is paramount as the interconnecting layers and different attachment sites in the fingers may lead to false negative findings.
For extensor tendon avulsion, image longitudinally over the DIPJ, looking for an avulsed bone fragment and hypoechoic retracted tendon that remains immobile during movement of the distal phalanx, the authors recommend. For central tendon slip injuries, image transversely over the middle phalanx to see the lateral slips moving below the midline axis of the PIPJ with finger flexion.