CT now has an important role in most kinds of cardiomyopathies, owing to its strength in morphological assessment and its ability to visualize calcium and coronary artery disease, according to a presentation at the International Symposium on Computed Tomography (ISCT 2016).
Dr. Hans-Christoph Becker, professor of radiology at Stanford University in California and former section chief for body CT at the Grosshadern campus of LMU/Munich in Germany, discussed how all four main forms of cardiomyopathies can benefit from CT, including the various permutations of normal, dilated, hypertrophic, and restrictive cardiomyopathy.
"If you think about cardiomopathy what first comes to mind in terms of a modality for imaging the disease is MRI, but ... I would like to show you the capability of CT to image the kind of diseases that are related to the muscle of the heart," he said. "As you know, there are different categories of cardiomyopathies including normal, dilated, hypertrophic, and restrictive cardiomyopathy, and in any of these disease entities CT can play a certain role."
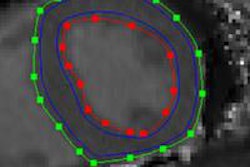
 Arrythmogenic right ventricular dysplasia at CT. All images courtesy of Dr. Hans-Christoph Becker.
Arrythmogenic right ventricular dysplasia at CT. All images courtesy of Dr. Hans-Christoph Becker.Dilated cardiomyopathies
Dilated cardiomyopathies are often characterized by enlarged ventricular cavities, with thinning of the myocardium down to < 1 cm. If CT images in systole are available, it's also worth looking at the mitral valve, which may show the nonapposition of the mitral valve leaflets as a sign of dilated cardiomyopathy and dilation of the myocardial valve ring.
"Of course, the real purpose of looking at cardiomyopathy with CT is not to study the myocardium but rather the coronary arteries -- and this is a pretty easy task because these patients tend to have low ejection fractions and the hearts beat very slowly, so the images tend to be of very good quality," Becker said.
Also, CT has proved useful for distinguishing ischemic from idiopathic cardiomyopathy, and CT can be as accurate as cardiac catheterization in distinguishing patients with idiopathic cardiomyopathies, just based on visualization of the coronary arteries, he explained. Thus, ischemic cardiomyopathy cases were distinguished by extensive coronary disease.
In one case Becker showed, acute myocardial infarction was characterized by low attenuation indicating lack of contrast uptake or edema, while chronic myocardial infarction manifested as myocardial thinning.
Investigators have looked at delayed myocardial enhancement too. Generally, they've found that CT doesn't do nearly as good a job as MRI, but that under certain circumstances it has a good ability to visualize myocardial infarction.
Restrictive cardiomyopathy
A case of restrictive cardiomyopathy showed extensive calcifications in the myocardium, which occurs fairly commonly and due to a range of causes, Becker said, noting a 2014 paper by Nance et al that clearly categorized the various differential diagnoses for findings of calcifications in the myocardium. One is dystrophic myocardial calcification caused by tissue damage due to ischemia, trauma, inflammation, or infection, or by tumor disease infiltration.
"More and more what I'm seeing is caseous microvalve calcifications, and it's interesting for me to see every second week in our unit," he said.
The other category where microcalcifications may occur is in impaired or distorted calcium metabolism due to reasons including secondary hypoparathyroidism, or lack of compliance with medication or dietary recommendations. In rare cases, the patient may have exaluria or vitamin D deficiency.
"Any of these reasons can be multifactorial and idiopathic, and once in a while the reason may be unclear," Becker said.
For example, a patient with end-stage renal disease had secondary hyperparathyroidism due to lack of compliance with medication or dietary restrictions; radiography showed extensive calcifications in the bones of the hand, with corresponding changes visible in the heart where extensive calcifications in the myocardium were associated with extensive pericardial effusion.
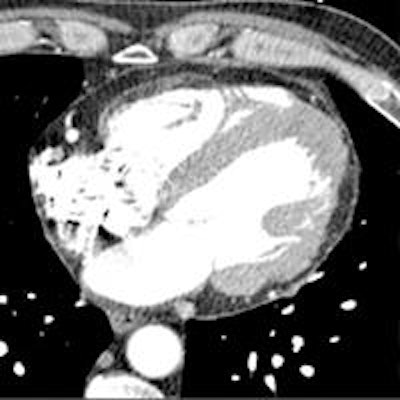
In a recent case from Stanford, myocardial calcifications were an incidental finding in a patient scheduled for aortic valve replacement.
"Unfortunately, I cannot provide a final diagnosis as to why the patient has so much calcium in the myocardium, but know it is certainly not secondary hyperparathoroidism because the creatinine was normal," Becker said. "My assumption is that this is of infectious origin."
 Patient scheduled for aortic valve replacement was found to have significant calcification in the myocardium of unknown etiology.
Patient scheduled for aortic valve replacement was found to have significant calcification in the myocardium of unknown etiology.Another incidental finding occurred in a patient being readied for a transcatheter aortic valve replacement (TAVR). However, instead of aortic disease he was found to have hypertrophic obstructive cardiomyopathy. CT is very helpful because this disease requires a very morphologic diagnosis, in this case showing a mass of soft tissue in the myocardium in the territory of the aortic outflow track as an indicator of hypertrophic obstructive cardiomyopathy.
Becker added that when he worked at the University of Munich, such patients were treated with septal alcohol ablation in a procedure where alcohol was mixed with the contrast media, enabling the radiologists to determine after the procedure exactly where the infarct had been induced.
"CT is very good for morphology in general, and this also applies to patients who are having myocardial noncompaction, which is diagnosed the same way in CT that it is in MRI," he explained. When the ratio of noncompacted to compacted tissue reaches 3 to 1, the patient can be diagnosed with noncompaction syndrome.
"To sum it up, CT seems to play a good role in a number of different entities in cardiomopathy," Becker said. "In dilated cardiomyopathy, the primary purpose of imaging in these patients is to look into the coronary arteries, and this is a pretty simple and straightforward task."
In hypertropic cardiomyopathy, it's advisable to perform a retrospective ECG-gated scan in order to have images from the entire cardiac cycle available for analysis, because there's a functional component to analyze more in detail. Finally, in restrictive cardiomyopathies it is advisable to perform prospectively ECG-triggered scans in order to visualize the extent of disease.