Cardiac MRI (CMR) can diagnose arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) where other modalities fail, and it can even identify conditions that mimic the disease -- good news considering that timely treatment can often prevent sudden cardiac death.
Researchers from the U.K. and Italy examined more than 1,000 patients referred for ARVC/D, and identified a handful of cases and more than twice as many phenotypes, or mimics, where other modalities like echocardiography were not definitive.
 Dr. Antonio Amadu from the Bristol Heart Institute and the University of Sassari.
Dr. Antonio Amadu from the Bristol Heart Institute and the University of Sassari."CMR was able to identify an underlying diagnosis in ... 14% of patients where other conventional techniques including ECG and echocardiography were inconclusive," Dr. Antonio Amadu from the Bristol Heart Institute and the University of Sassari in Sardinia, Italy, told attendees at last month's ECR 2016 in Vienna.
ARVC/D is a genetic heart disease usually transmitted via an autosomal pattern. Although it primarily involves the right ventricle, in rare cases it can encompass both sides of the heart. ARVC/D is typically characterized by partial or total absence of the right-ventricle musculature, which may be replaced by fibrofatty tissue, he said.
The clinical symptoms are often heterogeneous and nonspecific, and may include palpitations, syncope and atypical chest pain. As many as 23% of ARVC/D patients succumb to sudden cardiac death before they can be treated.
"Implantation of a cardiofibrillator decreases the risk of sudden cardiac death, so early diagnosis is crucial," Amadu noted in his talk.
The study analyzed CMR registry data for all of 2014 at the Bristol Heart Institute, and identified patients referred for suspected ARVC/D who were referred based on symptoms, clinical presentation, family history of ARVC/D, or family history of sudden cardiac death or abnormal transthoracic echocardiography.
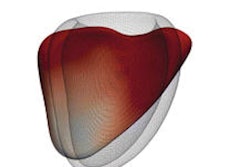
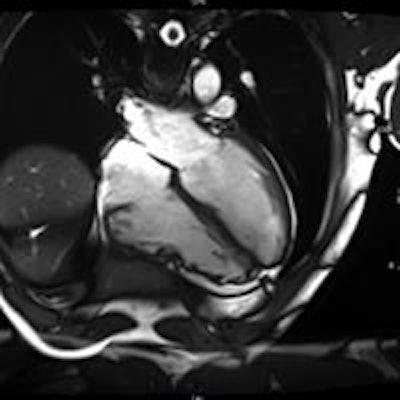
 Above and below: Patient with ARCV/D confirmed with CMR. All images courtesy of Dr. Antonio Amadu.
Above and below: Patient with ARCV/D confirmed with CMR. All images courtesy of Dr. Antonio Amadu.They identified 124 patients with suspected ARCV/D. This group had a median age of 40 years (± 16, range 17 to 77 years), representing 5% of total CMR referrals.
Amadu and colleagues from both institutions including Dr. C.L. Rodrigues, Dr. A. Dastidar, Dr. G.B. Meloni, Dr. M. Conti, Dr. Chiara Bucciarelli-Ducci et al, performed CMR on a 1.5-tesla scanner (Magnetom Avanto, Siemens Healthcare). A comprehensive protocol, including long and short-axis axial cine images and late gadolinium enhancement, was used in all patients.
CMR was able to identify an underlying diagnosis in 17 of 124 (14%) of patients, where other conventional techniques including ECG and echo, were inconclusive.
In all, four of the 124 patients met the CMR criteria for ARCV/D. Of these, three had major criteria and one had minor criteria, for a prevalence of 3%.
However, 11 patients or 9% had conditions that mimicked ARVC/D, including:
- Congenital absence of pericardium
- Asymmetric pectus excavatum
- Atrial septal defect with left or right shunting
- Arrythmogenic left ventricular cardiomyopathy
- Athletic heart (two)
- Left ventricular noncompaction cardiomyopathy
- Sarcoidosis
"CMR plays an important role in patients with suspected ARVC/D," Amadu said. Importantly, it can identify conditions that mimic the disease, representing 9% of the population studied, he added.
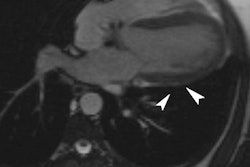
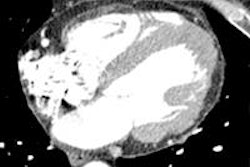
 Above: Anomalous venous return can mimic ARVC/D. (A) In four-chamber view, right ventricle dilated; (B) left, upper pulmonary vein on the left side of aortic arch (arrow) draining upwards toward the brachiocephalic trunk. Below: Atrial septal defect can mimic ARVC/D. Large superior interatrial defect is seen with blood flowing from the left to the right atrium (arrow).
Above: Anomalous venous return can mimic ARVC/D. (A) In four-chamber view, right ventricle dilated; (B) left, upper pulmonary vein on the left side of aortic arch (arrow) draining upwards toward the brachiocephalic trunk. Below: Atrial septal defect can mimic ARVC/D. Large superior interatrial defect is seen with blood flowing from the left to the right atrium (arrow)."Correct diagnosis of the underlying pathologies is pivotal, given its subsequent impact on clinical management and prognosis," Amadu said.