Follow-up FDG-PET scans can determine which patients with neuroendocrine tumors are suffering from progression of their disease and which of them would benefit from a change in therapy, according to an Austrian study published in the August issue of the European Journal of Nuclear Medicine and Molecular Imaging.
The findings from researchers at Innsbruck Medical University confirm that positive FDG-PET images "strongly correlated" with a higher risk of neuroendocrine disease progression in a direct comparison with gallium-68 (Ga-68) DOTATOC PET, based on both modalities' ability to detect somatostatin receptors (SSTR) on cell surfaces, which are linked to neuroendocrine tumors (EJNMMI, August 2016, Vol 43:9, pp. 1585-1592).
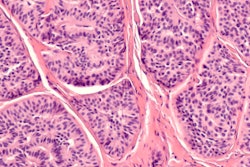
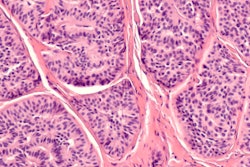
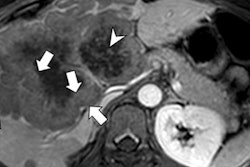
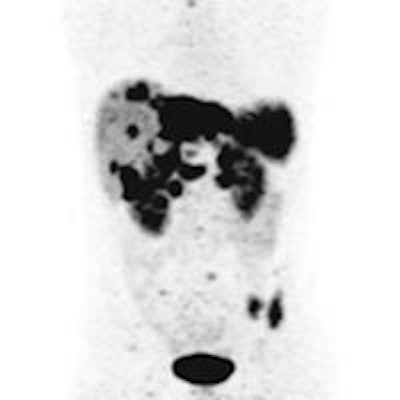
 PET images show a 32-year-old man with a grade 2 neuroendocrine tumor in the pancreatic tail. There were positive Ga-68 DOTATOC PET and FDG-PET results in both initial scans and during follow-up, which indicated disease progression. Images courtesy of EJNMMI.
PET images show a 32-year-old man with a grade 2 neuroendocrine tumor in the pancreatic tail. There were positive Ga-68 DOTATOC PET and FDG-PET results in both initial scans and during follow-up, which indicated disease progression. Images courtesy of EJNMMI."We recommend performing FDG-PET in the initial evaluation and during follow-up of neuroendocrine tumor patients, especially when SSTR PET/CT shows progression," wrote lead author Dr. Bernhard Nilica and colleagues from the departments of nuclear medicine and radiology. "FDG-PET/CT is a clinically relevant, complementary tool to [Ga-68] DOTATOC PET and its use represents a step towards personalized medicine in the management of neuroendocrine tumor patients."
FDG-PET doubts
The researchers cited previous papers in which SSTR imaging with a Ga-68-labeled peptide and PET/CT offers excellent sensitivity and specificity for diagnosing and staging neuroendocrine tumors. FDG-PET, of course, has been a mainstay for decades for oncology imaging, but the authors noted its use in neuroendocrine tumors is a "matter of controversy."
Several past studies, albeit with small cohorts, "cast doubt" on FDG-PET's efficacy in this patient population because less SSTR expression coincided with an increase in FDG glucose uptake.
"Consequently, it was suggested that the use of FDG-PET be limited to SSTR-negative neuroendocrine tumors," Nilica and colleagues noted.
Patients with neuroendocrine tumors are generally treated with peptide receptor radionuclide therapy (PRRT) followed by Ga-68 DOTATOC-PET to evaluate the status of somatostatin receptors. This approach is "preferable, because of its superior resolution and hence better sensitivity than that of conventional scintigraphy," the authors added.
Thus Nilica and colleagues sought to compare Ga-68 DOTATOC-PET and FDG-PET by retrospectively evaluating 66 patients who were treated with peptide receptor radionuclide therapy after the discovery of SSTR-positive lesions. Subjects underwent three combined imaging studies with Ga-68 DOTATOC and FDG-PET/CT at the hospital between 2005 and 2013.
The 38 males and 28 females with a mean age of 57.2 years (± 7 years) were in advanced stages of the disease, and more than 65% of the patients had metastases in more than one location. In fact, most of the subjects had widespread metastases. The average time from initial diagnosis to radionuclide therapy was 3.8 years (range of one to 11 years).
Ga-68 DOTATOC PET/CT was performed prior to PRRT, three months after first full treatment cycle, and every six to nine months thereafter. Ga-68 DOTATOC and FDG-PET/CT were performed on all patients within two months of each other, with an FDG-PET/CT scan included in a subject's routine work-up before PRRT. There was no therapy between the two imaging exams.
Clinicians performed a total of 198 combined Ga-68 DOTATOC and FDG-PET/CT studies from baseline to post-PRRT, with follow-up ranging from 11.8 to 80 months (mean of 34.5 months).
Patient analyses
Among the 66 patients in the study, three people (4%) had a complete response to radionuclide therapy. There was a partial remission in four cases (6%), stable disease for 35 patients (53%), and progressive disease in 24 cases (37%). All patients showed SSTR-positive tumor lesions at baseline and follow-up after the first round of PRRT.
Nilica and colleagues conducted a patient-based analysis that divided subjects into four groups based on whether FDG-PET and Ga-68 DOTATOC results were positive and/or negative at baseline and follow-up scans.
Within the comparisons, FDG-PET discovered more and/or larger metastases than Ga-68 DOTATOC-PET in five patients in the group of patients with both positive baseline and follow-up FDG-PET images, indicating disease progression. In this group, FDG-PET was positive for eight primary tumors in eight patients and for 44 metastatic lesions in 24 patients.
When Ga-68 DOTATOC-PET was positive both before and after treatment, the modality found nine primary tumors in nine patients and 55 metastatic sites among 24 patients. Ga-68 DOTATOC-PET also showed more metastases than FDG-PET in 11 patients, which included three patients with stable disease and eight cases of disease progression.
When baseline scans were negative and follow-up results were positive, FDG-PET showed more and/or larger metastases than Ga-68 DOTATOC-PET in four patients, all of whom had disease progression.
FDG-PET was positive for three primary tumors in three patients and 12 metastatic sites in nine patients. Positive Ga-68 DOTATOC-PET was seen for three primary tumors in three patients and 13 metastatic sites in nine patients. Tumors were grade 1 in two patients, grade 2 in six patients, and grade 3 in one patient, with no indication of disease progression.
'Important finding'
"This study confirmed that FDG positivity is strongly correlated with a higher risk of progression ... showing that FDG-PET has a prognostic value for early tumor progression," the authors concluded. "Furthermore, an important finding of our investigation is the evidence that patients may develop FDG-positive lesions during follow-up. This finding supports the value of repeating FDG-PET in the long-term follow-up of neuroendocrine tumor patients, in particular if there are signs of progression on other imaging methods such as SSTR PET/CT."
Given FDG-PET's performance, Nilica and colleagues added the evaluation of somatostatin receptors by Ga-68 DOTATOC PET/CT may not accurately reflect disease progression in certain neuroendocrine tumor lesions. Therefore, decisions on a treatment for a patient with a poor prognosis cannot be based only on Ga-68 DOTATOC-PET/CT results.