Grating inferometry phase-contrast imaging substantially outperformed x-ray absorption in the imaging of vulnerable coronary plaque, according to new research from University Hospital Zurich.
In an experimental coronary artery imaging setting, the image quality of vulnerable plaques obtained from cadavers was far superior to that of absorption imaging, characterizing plaques accurately in nearly 90% of vessels versus 18% for absorption imaging, the researchers said.
"Phase-contrast imaging is a reliable technique allowing for the accurate detection and characterization of coronary artery plaques," concluded Dr. Sebastian Winklhofer in a presentation at the RSNA 2014 meeting.
 Dr. Sebastian Winklhofer from University Hospital Zurich.
Dr. Sebastian Winklhofer from University Hospital Zurich."Phase-contrast imaging has recently ventured into many areas in radiology, promising results, for example, in breast cancer imaging, cardiovascular imaging, and skeletal imaging," he said in his presentation, adding that in breast imaging it has progressed to clinical use but has not yet been researched for coronary artery disease in human coronary arteries.
The study aimed to investigate the use of grating interferometry phase-contrast (PC) imaging for the characterization of human coronary artery plaques. The PC technique used in the study is based on measuring the phase shift of x-rays that occurs when the rays pass through an object, whereas absorption imaging measures x-ray absorption, he explained. A key benefit of phase-contrast imaging is its high sensitivity to electron density, which improves soft-tissue contrast versus absorption imaging.
In patients with vulnerable coronary artery plaques, determining plaque composition is probably more important than the degree of stenosis, as vulnerable or unstable plaque accounts for the majority of adverse cardiovascular events, Winklhofer said. Early identification is therefore key to predicting risk and preventing adverse events.
Using an experimental phase-contrast scanner setup that "took up the whole room," the study team used a synchrotron radiation source to perform ex-vivo imaging in coronary arteries taken from nine cadavers. Both absorption imaging and phase-contrast imaging was performed by two radiologists who were blinded to the results.
The analysis included a qualitative assessment and an assessment of plaque components like smooth muscle cells, collagen, and calcifications, and plaque classification according to American Heart Association guidelines, he noted. The HU of the various plaque components were assessed using region-of-interest measurements. The group performed quantitative measurements of the various plaque components, including collagen, lipid, smooth muscle, and calcification and compared them between phase-contrast imaging and absorption using analysis of variances (ANOVA) for repeated measures with a post hoc Bonferroni correction.
Phase-contrast outperforms
Subjective image quality was rated significantly higher for PC as compared with absorption imaging (P < 0.001). The intraclass correlation coefficient was excellent (0.89 for PC and 0.92 for absorption imaging, both P < 0.001).
For characterizing plaque composition, however, phase-contrast imaging correctly determined the composition in 33 of 38 plaques (87%) (Κ = 0.81; p < 0.001). On the other hand, absorption imaging allowed for the differentiation of calcified and noncalcified plaques just 18% of the time.
Moreover, the HU values of plaque components were significantly different at phase-contrast imaging (p < 0.05), but at absorption imaging "we did not find any [HU] differences between collagen or lipid or smooth muscle cells," (p = 1.00), Winklehofer said. Finally, phase-contrast imaging characterized early versus advanced lesions in all plaques (Κ = 1.00; P < 0.001).
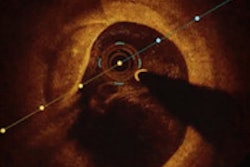
Winklehofer showed several examples of phase-contrast imaging, revealing high levels of anatomic detail visible in an intimal santoma, including the intima media and adventitia in the vessel wall. An image from a later stage of plaque development showed extracellular lipid accumulation that was readily visible in phase-contrast imaging.
"The next stage is a thin fiber atheroma, which has only a very thin cap," Winklhofer said. "There are diffuse tiny calcifications which are also very visible in the absorption images."
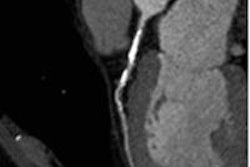
 Figure demonstrates an early fibrous plaque. Top row: Phase contrast image; absorption image; histopathology including Masson's trichrome (dark blue), Elastic van Gieson (red image), Hematoxylin, and Eosin stainings (light blue). Bottom row: Zoomed in phase contrast image and zoomed in histopathologic image to demonstrate the good visibility of the three vessel layers in phase contrast imaging. All images courtesy of Dr. Sebastian Winklhofer.
Figure demonstrates an early fibrous plaque. Top row: Phase contrast image; absorption image; histopathology including Masson's trichrome (dark blue), Elastic van Gieson (red image), Hematoxylin, and Eosin stainings (light blue). Bottom row: Zoomed in phase contrast image and zoomed in histopathologic image to demonstrate the good visibility of the three vessel layers in phase contrast imaging. All images courtesy of Dr. Sebastian Winklhofer.Phase-contrast imaging is a reliable technique for the detection and characterization of coronary artery plaques, he concluded.
The phase-contrast images "demonstrate excellent agreement with pathology, and the various components can be quantitatively differentiated with the HU," Winklhofer said. "This might allow for noninvasively improving the understanding of high-risk plaque development in patients suffering from coronary artery disease and also for identifying the patient at risk."