Gastric cancer remains a major cause of cancer-related morbidity and mortality worldwide, despite extensive screening programs and improved therapeutic strategies, but CT gastrography is beginning to show significant promise in the battle against this disease.
Research from South Korea, published by European Radiology on 1 October in an online first article, has confirmed that when 64-slice systems are used, the technique produces good diagnostic results for determining the depth of mural invasion in patients with gastric cancer. It can be particularly helpful for detecting early gastric cancer, and 64-slice CT is also useful for determining the T staging of gastric cancer, the researchers stated.
"As compared to conventional CT, the ability of multidetector CT to produce multiplanar reformatted images and 3D images, such as virtual gastroscopy, has been shown to improve the diagnostic accuracy of the detection and staging of gastric cancer, and especially early gastric cancer," noted Dr. Jin Woong Kim, Dr. Sang Soo Shin, and their co-authors from the department of radiology at Chonnam National University Hospital in Gwangju.
The researchers undertook a retrospective study to evaluate the accuracy of CT gastrography for determining the depth of mural invasion in patients with gastric cancer. CT scans were performed using a 64-slice system (LightSpeed, GE Healthcare). Before the scan, 10 mg of butylscopolamine bromide (Buscopan, Boehringer Ingelheim) was injected intramuscularly to minimize the peristaltic bowel movement and relax the bowel wall. Two packs of effervescent granules (Taejoon Pharmaceuticals) with a small amount of water were administered orally to distend the gastric lumen.


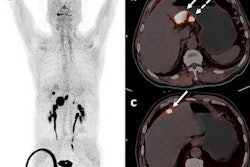
 Above: Axial CT image shows questionable thickening and enhancement of inner mucosal layer (arrow). Bottom left: Virtual gastroscopic image clearly shows ulcerative lesion with abrupt termination of folds at the same location as axial CT image. Bottom right: Conventional gastroscopic image reveals a malignant ulcer with abrupt termination of gastric folds. This lesion was diagnosed as early gastric cancer on biopsy. Images courtesy of Dr. Jin Woong Kim and Dr. Sang Soo Shin.
Above: Axial CT image shows questionable thickening and enhancement of inner mucosal layer (arrow). Bottom left: Virtual gastroscopic image clearly shows ulcerative lesion with abrupt termination of folds at the same location as axial CT image. Bottom right: Conventional gastroscopic image reveals a malignant ulcer with abrupt termination of gastric folds. This lesion was diagnosed as early gastric cancer on biopsy. Images courtesy of Dr. Jin Woong Kim and Dr. Sang Soo Shin.The degree of gastric distension was considered to be adequate when the gastric lumen was distended greater than 50% of the expected maximal luminal distension. Single-phase (portal venous phase) contrast-enhanced CT was performed after intravenous injection of 100 to 150 mL of iodinated contrast material with a power injector (Empowered CTA, E-Z-EM) at a rate of 3 mL/sec through an antecubital vein. The total amount of injected contrast material was adjusted according to the body weight of the patients (2 mL/kg).
Overall, gastric cancer was identified in 123 (96.9%) of the 127 cancers on the CT images. Four undetectable cancers on CT were pathologically staged as T1a (n = 3) and T1b (n = 1), respectively. In cases of early gastric cancer (EGC), 56 (73.7%) of the 76 cancers were visible on both the 2D and the 3D images, whereas EGC was identified only on the 2D and the 3D images in two (2.6%) and 14 (18.4%) cancers, respectively.
"All the AGCs [advanced gastric cancers] were visualized on both the 2D and the 3D images. With respect to the pattern of the gastric mural layering at the site of the gastric cancer and the adjacent normal gastric wall, among 109 gastric cancers that were detected on the 2D images, five (4.6%) and 104 (95.4%) cases were classified as single-layered and multilayered, respectively," the authors wrote.
Most patients (95.4%) showed a multilayered structure of the gastric wall around the lesion site. This observation may be because the gastric wall infiltrated by the tumor becomes thickened and/or stiff, which may negatively affect the distensibility at the site of the gastric cancer and the adjacent normal gastric wall. Alternatively, tumoral infiltration into the gastric wall may be accompanied by inflammatory or edematous change beneath the cancer, which may result in the exaggeration of the multilayered structure of the gastric wall.
This study had several limitations, the authors conceded. First, the patient population had heterogeneous repartition among different T stages, with more than 50% of patients having a T1 lesion. Second, the diagnostic criteria that were used for the T staging of gastric cancers in this study were quite different from previous studies. "Given that our new multidetector CT criteria were not yet widely accepted, the results of our study need to be cautiously interpreted," they wrote.
Also, the reviewers were aware of the conventional endoscopic findings with respect to the location of the lesion, which could have played a significant role in enhancing the detection rate of gastric cancer on the CT images. Finally, the study did not include lymph node staging because the radiologists focused on the diagnostic performance of multidetector CT for T staging according to the revised TNM staging system.
The researchers are now planning to perform several subsequent studies to assess the validity of new multidetector CT criteria for the T staging of gastric cancer.