VIENNA - Researchers from University Hospital Essen in Germany have shown the feasibility of whole-body staging of patients with neuroendocrine tumors with PET/MRI and the radiotracer gallium-68 (Ga-68) DOTATOC, and with greater reliability than PET/CT, in a preliminary study presented Friday at ECR 2013.
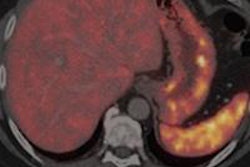
The preliminary results also illustrated the superiority of PET/MRI with Ga-68 DOTATOC in detecting malignant liver lesions compared with PET/CT, and the potential for whole-body PET/MRI with Ga-68 DOTATOC to replace PET/CT as the current gold standard in staging neuroendocrine tumors.
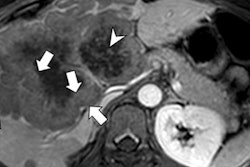
"Since liver metastases that originate from neuroendocrine tumors are hypermaterialized, the importance of a triple-phase contrast-enhanced protocol as part of a PET/CT scan has been emphasized in recent years," said lead study author Dr. Karsten Beiderwellen from the department of diagnostic and interventional radiology and neuroradiology. "However, we know that MRI offers special advantages in the detection of small liver metastases and bone metastases."
For that reason, he added, many groups have tried to fuse MRI and PET/CT images to create a retrospective PET/MR image of those small bioregions.
Patient sample
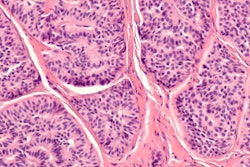
This study enrolled 30 patients (18 males and 12 females) with histologically confirmed neuroendocrine tumors and who were scheduled for routine PET/CT scans (Biograph mCT 128, Siemens Healthcare) with Ga-DOTATOC.
All the participants underwent a triple-phase contrast-enhanced protocol, but no contrast agents were administered in two patients who had suffered renal failure.
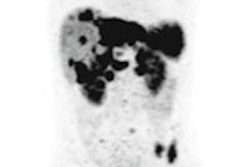
Subsequently, all patients received a whole-body PET/MRI (Biograph mMR, Siemens). The scan protocol include T1-weighted pre- and post-DOTATOC scans, T2-weighted half-Fourier acquisition single-shot turbo spin-echo (HASTE) sequence, and coronal short-tau inversion recovery (STIR) sequence, diffusion-weighted MR imaging (DWI), and a dynamic liver series.
The resulting datasets were rated by two radiologists who counted the number of lesions, their locations, and characterizations on a four-point scale, with 0 as not visible and 3 as malignant. The study specified five lesions per organ and used prior PET/CT and PET/MRI exams and clinical follow-ups as reference standards.
All available PET/CT, PET/MRI, and historical data and clinical follow-up (mean of 95 days) served as standards of reference.
When the detection rates for each modality were calculated, researchers found 19 (63%) of 30 patients had malignant lesions. PET/CT was able to correctly identify 17 (89%) of the 19 malignant lesions, while PET/MRI identified all 19 lesions (100%).
A total of 186 lesions were discovered, with 137 lesions (74%) being malignant and 49 (26%) lesions being benign. PET/CT correctly identified 124 malignant lesions (90%), while PET/MRI again correctly identified all 137 malignancies (100%).
Liver metastases
The review of images also found 80 liver metastases in patients. PET/CT correctly identified 68 (85%) of the liver metastases as malignant. Of the remaining malignant lesions, eight lesions were too small to characterize on CT and four lesions were not detected at all. By comparison, PET/MRI again correctly identified all the lesions as malignant.
Correct identification of all malignant neuroendocrine tumor lesions with PET/MRI was possible, while PET/CT "remained inconclusive" in several cases, Beiderwellen concluded. PET/MRI also discovered 12 additional liver metastases not detected by PET/CT.
He added that the scan time for PET/MRI may be a potential downside. "A PET/MRI examination still takes a lot longer than PET/CT, if there is an extensive protocol, such as ours," Beiderwellen said. "This protocol took 70 minutes, so we have to identify redundant sequences to shorten the protocols."
In addition, MRI is "not the reference method for the depiction of lung metastases, so it has to be further evaluated," he noted.