New research shows coronary artery calcification (CAC) is a frequent incidental finding in middle-aged adults undergoing chest CT, with more than 25% of CAC patients having moderate to severe disease, according to a presentation at the recent European Society of Cardiovascular Radiology (ESCR) annual congress in Antwerp, Belgium.
In a study involving patients between the ages of 40 and 69, the reporting radiologist mentioned the presence of CAC in only 35% of cases, which is slightly lower than in other studies, but a relatively low number of unreported CAC was categorized as moderate or severe disease, noted Dr. Veronika Majcher, specialty registrar in radiology, and her colleagues at Cambridge University Hospitals National Health Service (NHS) Foundation Trust.
"The traditional management of moderate and severe coronary artery calcification based on the Agatston categories includes aggressive risk factor modification, with additional functional testing often guiding decisions for revascularization," they told ESCR delegates. "This makes reporting of coronary artery calcification critical and may enable immediate change in patient management."
While much less frequent, aortic valve calcification can be significant in up to a third of positive cases in this age group, continued the authors. Previous studies have shown that an aortic valve Agatston score above 150 may warrant echocardiographic evaluation, while a score above 500 should lead to echocardiographic assessment for aortic stenosis.
Development of CAD
Coronary artery disease (CAD) is the single biggest cause of cardiac morbidity and mortality, while calcific aortic valve stenosis (AVS) is the third leading cause of cardiovascular disease. This places a major burden on healthcare systems, they noted.
CAD develops as a chronic process of atherosclerotic plaque formation with progressive luminal narrowing. The natural history of these plaques varies, but most will form and evolve over years to decades, with atheroma remodeling and calcification, before any symptoms develop, according to Majcher and colleagues. Similarly, AVS often develops and progresses silently, and by the time symptoms are present, the prognosis is poor.
"The increasing number of CT chest examinations presents an opportunity to 'screen' a large number of asymptomatic individuals for coronary artery and aortic valve disease," they explained. "A hallmark of both atherosclerotic CAD and AVS is the development of calcification."
The degree of CAC on CT is a well-validated marker of total coronary artery atherosclerotic burden, and CT measures of aortic valve calcification correlate with the severity of aortic stenosis and can provide useful extra information. The Agatston method for quantifying CAC on electrocardiogram (ECG)-gated CT scans has been extensively validated and, more recently, a visual approach has been proposed for quantifying CAC on non-ECG-gated studies, they added.
Main research goals
The aim of the Cambridge group's study was to assess the incidence and severity of coronary artery and aortic valve calcification on non-ECG-gated chest CT. The team also evaluated the correlation between the visual and Agatston scores for coronary artery and aortic valve calcification. Additionally, they investigated whether these findings were mentioned in the CT reports.
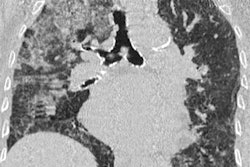
Their single-center retrospective study included 400 consecutive unenhanced non-ECG-gated chest CT examinations of patients between the ages of 40 and 69 over a period of three months. Exclusion criteria included previous cardiac intervention (coronary stent, coronary artery bypass graft, or valve replacement) and repeat scans in this time period. All scans were performed using volumetric acquisitions with slice thickness of 1 mm on a multislice CT scanner. The kV median and interquartile range was 120 (120-130) and mA adjusted, depending on patient factors. The mediastinum window (width, 400; level, 40) was used for analysis.
Data analysis included the comparison of visual score results of the ordinal method determined by one observer and the Agatston score calculated with syngo.via software (Siemens Healthineers) by a second observer. Both were blinded to the results of the other method. The Spearman rank correlation coefficient was calculated to describe the relationship between these two methods of calcium score assessment.
| Presence of CAC and/or AV calcification in middle-aged adults | ||||
| Variable | Coronary artery calcification | Aortic valve calcification | Total | |
| (+) AV calcification | (-) AV calcification | (-) Coronary calcification | ||
| Female | 19 (11%) | 52 (31%) | 4 (2%) | 75 (44%) |
| Male | 17 (10%) | 74 (44%) | 3 (2%) | 94 (56%) |
| Total | 36 (21%) | 126 (75%) | 7 (4%) | 169 |
Out of the 400 consecutive chest CT examinations, 375 were eligible for inclusion in the study; 169 (45%) were positive for coronary artery and/or aortic valve calcification (see table), while 206 (55%) were negative for both.
The chest CT scans of 162 (43%) patients were positive for CAC, out of which 36 (10%) were also positive for aortic valve calcification; 71 (44%) patients were female and 91 (56%) were male. The total median age and interquartile range was 63 (57-67) years, which was similar in both genders, at 62 (57-66) years for women and 63 (56-67) years for men. The median visual score was 2 (1-4) and the median Agatston score was 95 (20-322).
The degree of calcium severity, as assessed by ordinal visual score, was found to be mild in 117 patients (72%), moderate in 28 (17%), and severe in 17 (11%), with more than a quarter showing moderate to severe calcification. In only 57 (35%) of the reports was the presence of coronary calcium mentioned by the reporting radiologist. Of the cases not reported, 87 (83%), 15 (14%), and three (3%) were in the mild, moderate, and severe categories, respectively.
A high degree of association was observed between the severity ranking of CAC by visual and Agatston scores, with 135 (83%) of severity rankings in the same category. The accuracy was 90%, 85%, and 91% in the mild, moderate, and severe CAC severity categories, respectively. This showed strong correlation (r = 0.82, p < 0.0001) between the visual and Agatston scores using the Spearman rank correlation coefficient.
Overall, this research demonstrates that visual scoring methods for coronary artery and aortic valve calcification can be used on unenhanced, nongated chest CT examinations, and that these correlate with formal scoring methods, according to the authors.
The main limitation of the study was the relatively small cohort in view of the high prevalence of coronary artery disease in the general population, but this was sufficient to allow the authors to make an initial assessment of the patient cohort and to obtain significant results about the methods for quantification. Additionally, they could not control for acquisition parameters due to the retrospective nature of the study, but the majority of the studies were performed at a standard 120 kV.
By providing the referring physician with a severity score for coronary artery and aortic valve calcification, further investigation may be prompted, which could lead to earlier intervention and improved outcomes for these patients, they concluded. The results should encourage routine reporting and quantification of coronary artery and aortic valve calcifications on non-ECG-gated CT chest exams.
If you'd like to see the authors' full range of clinical images and figures shown at ESCR 2019, you can view their presentation on the Electronic Presentation Online System (EPOS) section of the European Society of Radiology website.