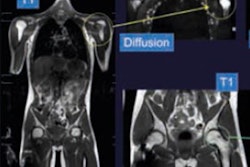
Coronal short tau inversion recovery (STIR) is the best MRI sequence for detecting bony and soft-tissue acute injuries to the hip, and anybody looking to create an abridged protocol should prioritize it over other sequences, new research has found.
"Reviewing the two coronal sequences when the patient is still on the scanner might obviate the need for further sequences, reducing the overall time of the scan," noted radiologist Dr. Christopher Lord and colleagues from Southampton General Hospital, U.K., in a presentation at the 2017 meeting of the European Society of Musculoskeletal Radiology (ESSR) in Bari, Italy.
An estimated 75,000 hip fractures occur in the U.K. every year, costing around 2 billion pounds (2.2 billion euros) in terms of health and social care. All-cause mortality following hip fractures is high; an estimated 10% of patients die within one month and two-thirds die within 12 months after the injury.
X-ray has 90% sensitivity for suspected hip fracture, but the prevalence of occult hip fracture ranges from 3% to 4% in patients presenting to the emergency department with acute hip pain, Lord explained.
"Early diagnosis is critical as a delay in surgical fixation confers negative outcomes," he said. "MR has been shown to be superior to other imaging modalities for the evaluation of occult bony injury and offers more comprehensive evaluation of associated soft-tissue abnormality. Scanner availability and the length of time to perform the conventional full hip protocol are the primary barriers to rapid MR access in our cohort of patients."
Boosting speed and efficiency
The Southampton group was keen to improve the speed and efficiency of its MR protocol for evaluation of acute hip pain. They wanted to devise an abridged protocol based on selected T1 and fluid sensitive imaging, whilst maintaining high levels of diagnostic accuracy. The aim was to reduce overall scan time and increase the availability of direct access to MRI in this group of patients.
The study population constituted consecutive patients undergoing MRI for acute hip pain with negative plain radiographs at a single major trauma center. The team retrospectively reviewed scans conducted between December 2013 and January 2017. Patients included had a minimum scan series of axial T1/STIR and coronal T1/STIR sequences, and those with alternate sequences or nondiagnostic imaging scans were excluded. A total of 49 patients met the above criteria (37 women, 12 men, mean age 78, and age range 34 to 96).
All scans were performed at 1.5-tesla. Studies were divided into individual sequences (axial T1, axial STIR, coronal T1, and coronal STIR) that were anonymized and randomized. A senior musculoskeletal resident and a fellowship-trained musculoskeletal radiologist with six years of experience were blinded to the examination report, prior radiographs, and scan indication. They evaluated the individual sequences for the presence of hip fracture, other pelvic fracture, and soft-tissue injury. Positive findings were classified by location, and the data were compared against the full examination to assess the sensitivity and specificity of each sequence.
Of the 49 patients, 77% (38/49) had positive scans for a traumatic bone or soft-tissue abnormality. Around 41% (20/49) patients had fractured proximal femora (11 intracapsular, 9 intertrochanteric), and 16% (8/49) had pelvic fractures. They were often multiple (three acetabular, seven ramus, seven pubic). A total of 67% of patients (33/49) had acute traumatic soft-tissue injuries, and commonly more than one muscle group was injured (27 adductors, 16 gluteals, five iliopsoas, five short external rotators, and 11 quadriceps).
| Coronal STIR sequence values | ||||
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
| Proximal femoral fracture | 100 | 100 | 100 | 100 |
| Pelvic | 94.1 | 100 | 100 | 96.8 |
| Soft tissue | 97.1 | 100 | 100 | 93.7 |
Lord and colleagues calculated the sensitivity, specificity, and positive and negative predictive values for each sequence. The coronal STIR sequence had the highest overall sensitivity and specificity for both proximal femoral and pelvic fracture. The axial T1 and STIR sequences were found to have equivalent performance for proximal femoral injury, but the axial STIR performed better than the axial T1 for pelvic fractures. The coronal T1 sequence was the least sensitive and specific for proximal femoral fracture, but was equivalent to axial T1 for pelvic injuries. This was due to bone marrow heterogeneity in the plane of the fracture, which may confound interpretation and in general reflects a potential pitfall with T1 imaging, they reported.
"Both STIR sequences outperformed T1-weighted imaging in the assessment of soft-tissue injuries, where T1 had very poor sensitivity in both planes. This is because the presence of intramuscular edema and fluid-related abnormality is not well seen on T1," the researchers wrote. "When positively identified on T1, associated soft-tissue injuries tended to be gross or demonstrate high signal hematoma, accounting for the relative high specificity."
Although T1-weighted imaging has poorer sensitivity than STIR imaging for both fracture and soft-tissue injury, inclusion of T1 sequence in the acute hip protocol remains important, and correlating the low T1 fracture line with bone marrow edema on fluid-sensitive sequences is essential to differentiate fracture and contusion, they added. The fracture line extension and potential involvement of the cortex are better visualized on T1. Also, T1 sequences are superior for characterization of the bone marrow to exclude malignant infiltration, which in subtle cases can easily be discounted as nonspecific signal heterogeneity on STIR imaging.
Final advice
The authors recommended that coronal STIR should be performed as the first and primary sequence in an abridged protocol, particularly for patients who are in pain and are at risk of abandoning the exam. In addition, a T1 sequence should be included in the minimum protocol for visualization of the fracture line and for marrow assessment.
"Although axial T1 performed better than coronal sequences for proximal femoral fracture in our series, we would nonetheless recommend inclusion of the coronal T1 in the first instance for better anatomical correlation with the coronal STIR," they wrote. "If an additional sequence needs to be performed, the axial STIR would be the next sequence to use due to its high sensitivity for fractures and soft-tissue injuries."
For free access to the authors' full range of clinical cases and images presented at ESSR 2017, which is available on the European Society of Radiology's EPOS database, click here. The co-authors of the study were Drs. S. Leach and V.T. Skiadas.