Automated segmentation algorithms that prepare CT images for 3D printing haven't advanced to the point where they can outperform humans setting threshold levels manually, concluded a new study in the International Journal of Computer Assisted Radiology and Surgery (IJCARS). As a result, 3D models emerge with fewer errors when threshold levels are set manually.
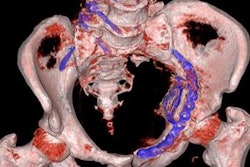
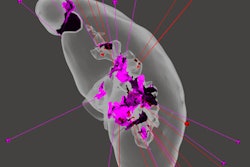
In the study, researchers from the Netherlands scanned one female and one male cadaver head with CT, conebeam CT, and dual-energy CT. The group manually thresholded all bony structures on the CT images, then used the highest and lowest mean threshold values to generate skull stereolithography (STL) models. Default thesholded models were then superimposed on an optical scan of the skulls. Manual threshold selection resulted in better STL models than default thresholding, they reported.
"The use of dual-energy CT and conebeam CT technology in its present form does not deliver reliable or accurate STL models for medical additive manufacturing," wrote lead author Maureen van Eijnatten and colleagues, a PhD candidate at the 3D Innovation Lab in VU University Medical Center (VUMC) in Amsterdam (IJCARS, 7 October 2016).
More development needed
New approaches based on pattern recognition and machine learning algorithms will be needed to properly segment these images without human intervention, the authors wrote.
Additive manufacturing or 3D printing combined with advanced imaging modalities such as CT or MRI has brought a paradigm shift to the creation of a wide range of patient-specific models including implants, saw guides, and drill guides designed to fit the specific anatomic needs of patients, the study team wrote. But CT images are acquired with a variety of technologies these days including single-source, dual-source, and conebeam CT models -- all of which produce slightly different grayscale profiles.
Three-dimensional printing requires the conversion of DICOM images into STL files before a model can be printed, and thresholding of CT values is the most common segmentation method. Thesholding results in all voxels with a gray value greater or equal than the chosen threshold value to be included in a segmented volume that uses a binary mask.
Medical image segmentation software packages offer only a single, default compression value for compact bone, soft tissue, and cartilage. And unfortunately, their default values aren't usually optimized for all types CT acquisitions, so they can't account for the variations in gray values between different scanners.
As a result, manual thresholding is usually still needed to create the optimal STL model, even though manual thresholding is a subjective task, particularly in the head area with all of its bony structures. Minor errors in the facial area can have a big impact on patient function and on the aesthetic appearance, the study team wrote.
Nor are there many clues in the literature to determine how well automated thresholding works versus the manual kind. Therefore, this study sought to assess the impact of both threshold selection types on the accuracy of skull STL models that were acquired using different settings and modalities.
The group scanned two preserved cadaver heads using three CT technologies including high-resolution 64-detector CT (Discovery CT750 HD, GE Healthcare), conebeam CT (NewTom 5G CBCT, NewTom), and Vatech PaX Zenith 3D conebeam CT (Vatech). The GE scanner was also operated in dual-energy imaging mode, resulting in images from four different modalities being produced.
After scanning, the corresponding DICOM files were imported into Osirix MD software (Osirix Foundation), a U.S. Food and Drug Administration (FDA)-cleared package that is commonly used in additive manufacturing. The software provides options for both manual and default threshold selection.
In a bid to graphically demonstrate the distribution of gray values in the manually selected and default threshold values, histograms were plotted for each of the four CT scanners using software (MatLab v.2012, MathWorks, Natick, Massachusetts, USA),
Manual thresholding favored
The results showed good intra- and interobserver variability for manual threshold selection, with intraclass correlation coefficients > 0.9, the authors wrote. All engineers selected gray values closer to soft tissue to compensate for bone voids, they wrote.
The results revealed variations between the automatic and manually thesholded STL models of the following:
- 0.13 mm for MDCT
- 0.59 mm for dual-energy CT
- 0.55 mm for conebeam CT
Moreover, all STL models showed inaccuracies ranging from -0.8 mm to + 1.1 mm (MDCT) to -0.7 mm to + 2.0 mm (DECT) and -2.3 mm to + 4.8 mm (conebeam CT), the study team reported.
Partial volume effect: An issue
The investigators purposely selected the soft-tissue threshold values during bone segmentation in order to include the maximum number of bone-specific gray values, which are allocated to voxels that represent different tissues during CT reconstruction, the authors wrote.
During this process, voxels on bone-to-soft-tissue boundaries that contain soft tissue are commonly assigned to a lower gray value than bone, a phenomenon known as partial volume effect (PVE). This can result in voxels being erroneously allocated to soft tissue rather than bone, resulting in bone voids and data loss.
"Therefore, engineers should be aware of this phenomenon since data loss can lead to large inaccuracies in individualized printed medical constructs," they wrote.
Some investigators, notably in CT colonography, have developed algorithms designed to minimize PVE in computer-aided detection (CAD) systems.
Overall, manual thesholding results in better STL models than default thresholding, the group concluded.
The use of dual-energy CT and conebeam CT technology in its current form does not offer reliable or accurate STL models for 3D printing, van Eijnatten and colleagues concluded. New approaches based on pattern recognition and machine learning algorithms will improve the process.
"Clinicians and engineers should keep in mind that the DICOM-to-STL conversion procedure, and particularly the threshold selection, is a critical step in creating an accurate 3D printed construct for medical purposes," Eijnatten wrote in an email.