In a population of myocardial infarction patients spanning 10 years of clinical practice, coronary CT angiography (CCTA) showed only limited ability to detect culprit lesions in the coronary arteries that went on to cause heart attacks -- though its positive predictive value was perfect, researchers concluded.
Investigators on both sides of the Atlantic had hoped to use CT to identify potential culprit lesions before invasive angiography was needed, considering that the noncalcified plaques visible on CCTA were the likeliest candidates representing the culprit lesions that go on to cause myocardial infarction. But among 2,500 patients scanned since 2005, including 59 chosen for analysis, CT demonstrated only a 60% sensitivity for detecting culprit lesions, though it had no false positives either.
The results underscore the superiority of intravascular ultrasound (IVUS) and invasive coronary angiography for vulnerable plaque detection, and they perhaps highlight the need for advanced CT techniques in this setting, researchers reported at ECR 2016 in March.
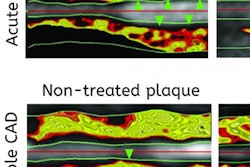
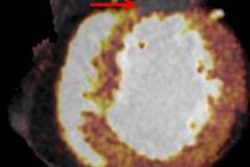
 Culprit plaque responsible for subsequent myocardial infarction in the left anterior descending artery. Image courtesy of Stephen Fuller and Dr. Damiano Caruso.
Culprit plaque responsible for subsequent myocardial infarction in the left anterior descending artery. Image courtesy of Stephen Fuller and Dr. Damiano Caruso."In our population, CT showed decreased accuracy for finding the culprit lesion, which can be explained by the positive population and the known relatively low positive predictive value of cardiac CTA," said research coordinator Stephen Fuller from the Medical University of South Carolina (MUSC). Dr. Damiano Caruso and colleagues from the University of Rome "La Sapienza" also collaborated on the study.
Focus on NSTEMI patients
The researchers specifically focused on patients with non-ST-elevation myocardial infarction (NSTEMI), who represent 60% to 70% of all myocardial infarctions because they lack the classic signs of ischemia on electrocardiogram (ECG) measurements, Fuller said. As a result, the condition is typically diagnosed by a combination of serum troponin and the patient's clinical presentation.
"Because the patients are less likely to go to cath immediately, there's an increased role for noninvasive studies like cardiac CT to identify culprit lesions and determine if intervention is warranted," he said.
The role of noncalcified plaque is well-documented in both the STEMI and NSTEMI populations using intracoronary measurements such as near-infrared spectroscopy (NIS) and invasive coronary angiography, but not CCTA.
Can CT identify the perpetrators?
The group screened a database of NSTEMI patients who had undergone prior cardiac CT to identify possible culprit plaques on CT and correlate the results with invasive angiography.
Plaque composition was noted by a reader who scored plaque severity on a scale of 0 to 3, with a plaque score of 2 or greater considered a culprit lesion. The team assessed and compared culprit lesions, and assessed the performance of culprit lesion composition as well as the diagnostic performance of CCTA.
Fuller and colleagues excluded patients with multiple bypass grafts or stenting, those with an intervention between cardiac CT and invasive angiography, and those whose tests were more than a year apart. A two-sided z-test was used to compare percentages.
The analysis included 944 vessel segments and evaluated 170 plaques. In all, 93 plaques were calcified, eight were classified as noncalcified, and 69 were classified as mixed.
Most of the noncalcified plaques were selected as the culprit lesion. In fact, the percentage of noncalcified plaques rated as the culprit lesion (63%) was significantly higher than the percentage of both calcified (20%) and mixed plaques (21%), the group reported.
Using invasive coronary angiography as the gold standard, CT revealed a sensitivity of just 60% for finding the culprit, with a specificity of 88%, Fuller said. At the same time, CCTA had a positive predictive value of 100% and a negative predictive value of 87%.
| Accuracy by modality in NSTEMI population | ||
| CCTA | Invasive coronary angiography | |
| Per-segment analysis | ||
| Occluded segments | 16 | 22 |
| Culprit lesions | 44 | 61 |
| Per-patient analysis | ||
| Occluded segments | 12 | 18 |
| Culprit lesions | 14 | 23 |
Although CT's ability to detect the culprit lesion was limited, it revealed a 100% positive predictive value with no false positives, Fuller said.
"This kind of makes sense in the context that this is a strongly positive population, because cardiac CTA has a known strong positive predictive value compared to its negative predictive value, and we would expect cardiac CT to have some deficiencies in detecting culprit lesions in a positive population," he said. "So our conclusion is that NSTEMI is associated with a diversity of risk factors, all of which were expected."
Study limitations included a relatively heterogeneous population and wide range of time, up to a year, between CCTA and invasive angiography, Fuller added. Over a 10-year study, CT scanners and protocols change often. And the sample size of culprit plaques was low, with a limited definition not necessarily confirmed by cardiology.
"Obviously, plaque characterization with quantitative analysis would produce better data," he said. "Quantitative plaque analysis with IVUS correlation if available would be an improvement, as well as comparing culprit arteries and plaques versus nonculprit plaques in the same patients, and integrating functional data including fractional flow reserve CT and comparing our group to a matched stable or coronary artery disease population."
The group also looked at the STEMI population, but the number of patients was very low.