Coronary CT angiography (CCTA) with a 256-detector-row CT scanner delivered better image quality, fewer artifacts, and a drastically reduced radiation dose compared with a 64-detector-row CT scanner, according to new research from France.
The study of 58 patients -- half scanned on a 64-detector-row machine and half on the 256-detector-row scanner (Revolution CT, GE Healthcare) -- also showed far fewer inaccessible coronary segments on 256-detector-row CT (17.8%) versus 64-detector-row CT at 1.5%. And nondiagnostic images due to motion artifacts occurred in only one patient with 256-detector-row CT, which also improved contrast-to-noise ratio (CNR) by one-third.
All of this was accomplished with an 81% drop in effective radiation dose -- down to a mean 2.7 mSv with the 256-detector-row machine -- the study team from Saint-Denis, France, reported.
"A new-generation, large-detector 256-detector-row scanner performing CCTA on high heart rate patients showed remarkable improvement in image quality combined with a large reduction in radiation dose in this preliminary study," Dr. Laurent Macron said in a presentation at ECR 2015.
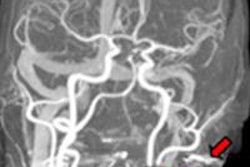
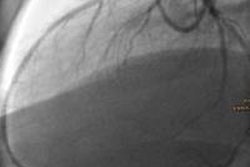
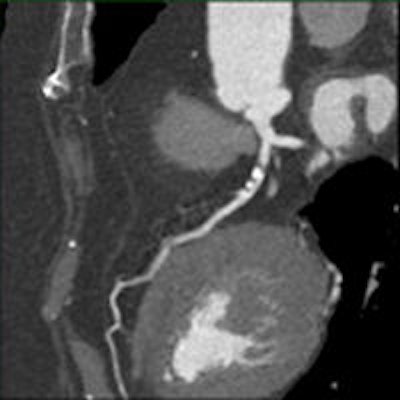
 Above: ECG trace showing one-beat cardiac examination; heart rate 87 bpm. Below: Angiographic view. Bottom: Curved and short-axis views demonstrating severe stenosis on left anterior descending (LAD) artery. All images courtesy of GE Healthcare.
Above: ECG trace showing one-beat cardiac examination; heart rate 87 bpm. Below: Angiographic view. Bottom: Curved and short-axis views demonstrating severe stenosis on left anterior descending (LAD) artery. All images courtesy of GE Healthcare.Several studies have concluded that 64-detector-row CT delivers high diagnostic accuracy, Macron said. At the same time, as many as 15% of the coronary segments imaged at CCTA may be nonassessible, according to one report -- "and the main reasons were severe coronary calcifications and motion artifacts, the latter occurring especially with high heart rates," said Macron, a radiologist from the Centre Cardiologique du Nord who is also a consultant for GE Healthcare.
According to standard guidelines, CCTA should not be performed in patients with heart rates of 65 beats per minute (bpm) or higher, but a new scanner might ultimately expand those limits. This study sought to show that 256-detector-row CT may improve the feasibility of coronary CTA in patients with high heart rates, "thanks to whole-heart coverage within one beat and high rotation speeds," Macron said.
The group retrospectively examined 58 patients with a heart rates higher than 65 bpm during CCTA. In all, 29 were scanned on 128-detector-row CT (group A) and 29 underwent the exam on 256-detector-row CT. (Both scanners are equipped with ultrafast kV switching, effectively making the 256-detector-row scanner a 512-slice machine, and the 64-detector-row scanner into a 128-slice machine.)
Two experienced readers evaluated image quality using a three-point scale (3 = no artifact; 1 = interference with diagnosis), and the importance of motion and step artifacts using a five-point scale (5 = no artifact). Finally, the study team calculated the percentage of assessable coronary segments, measured objective image quality, and calculated mean effective dose.
According to the results, the mean heart rate was similar between the two 29-patient cohorts: 73.3 ± 6.9 bpm for group A and 75.7 ± 9.9 bpm for group B.
But in group A, 16% of coronary segments were not assessable, with motion artifacts rated at 1.93 ± 0.74 and step artifacts at 2.27 ± 0.69, according to the study authors. For group B, the percentage of nonassessible segments fell to less than 2%, with no step artifact. Motion artifact for group B was rated at 2.41 ± 0.62.
At the same time, the mean effective dose in group B was reduced by 81% to 2.7 ± 2.4 mSv, versus 14.2 ± 4.4 mSv in group A (p < 0.001). Also, for group B the CNR increased by 32%.
On a per-patient basis, image quality rose significantly in group B (p < 0.001) with 256-detector-row CT, Macron said.
"Indeed, almost all of the patients with good or excellent image quality were 256-detector-row CT and only one patient had poor image quality," he said. "More than 95% of patients had good or excellent image quality in group B, and there was no misalignment artifact due to the wide detector that performed a whole-heart acquisition in a single beat and high rotations speeds."
Most important, Macron said, is that the improvement in image quality resulted in an improvement in coronary segment analysis. There were only six segments out of 406 that were not accessible in group B -- less than 2% -- compared with 17.8% in group A, and the improvement was observed regardless of the coronary artery being considered.
| Coronary segment accessibility, per segment analysis | |||
| Segment | 64-row CT (n = 406) |
256-row CT (n = 406) |
P-value |
| Right coronary artery (RCA) | 84% (98/116) | 100% (116/116) | < 0.001 |
| Left anterior descending (LAD) | 82% (119/145) | 97% (141/145) | < 0.001 |
| Left circumflex artery (LCX) | 81% (117/145) | 99% (143/145) | < 0.001 |
New-generation 256-detector-row CT enabled the performance of arterial CCTA on high-heart-rate patients with "remarkable improvements" in image quality and diagnostic accuracy, along with substantially reduced radiation dose in this preliminary study, thus paving the way for wider use of this exam, he said.
Still to be proved in future research are substantial improvements in diagnostic accuracy in this population of patients fast heart rates, Macron said.