Image guidance using motion-compensated digital tomosynthesis has the potential to improve targeting accuracy during treatment of lung cancer patients, according to researchers from The Netherlands Cancer Institute (NKI) in Amsterdam.
Stereotactic body radiotherapy (SBRT) is an alternative treatment option for patients diagnosed with stage 1 non-small cell lung cancer (NSCLC) who cannot or will not undergo surgery. Because of the high radiation dose that it delivers, SBRT requires high-precision treatment delivery. Motion compensation, however, can improve the quality of digital tomosynthesis images used to guide SBRT in lung cancer patients (Radiotherapy and Oncology 07 October 2013).
The challenge of volumetric-modulated arc therapy (VMAT)-based SBRT delivery to the lung is to compensate for inter- and intrafraction position variability and respiratory motion. Cone-beam CT (CBCT) scanning integrated with a linear accelerator is used to localize targets with high precision. But CBCT scans have limited capacity for patient surveillance during treatment delivery.
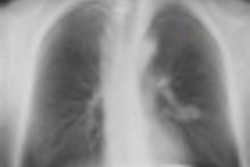
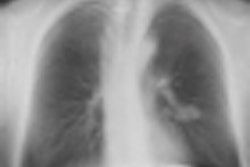
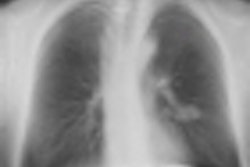
Digital tomosynthesis is a limited-angle image reconstruction method from 2D cone-beam projections that improves the visibility of patient anatomy compared with 2D images. The addition of motion compensation has the potential to improve the quality of digital tomosynthesis images by mitigating blur and other respiratory motion-generated artifacts.
To test this idea, Anneke van der Reijden and colleagues conducted a feasibility study using images of three patients who had received SBRT at NKI. Patients with different sized (smaller than 5 cm), peripherally located tumors that demonstrated considerable tumor motion on a pretreatment 4D CT scan were selected. The researchers reconstructed digital tomosynthesis images using the patient scans, as well as a respiratory motion phantom, with and without motion compensation.
 Anneke van der Reijden from the NKI's Department of Radiation Oncology.
Anneke van der Reijden from the NKI's Department of Radiation Oncology.
Motion-compensated digital tomosynthesis reconstruction was achieved by back projection over curved lines. The researchers first sorted the projection images according to their breathing phase using the Amsterdam shroud technique. Motion models derived from the 4D planning CT (4D Deformation Vector Field, DVF) were applied to curve the lines during back projection into a corresponding 30° digital tomosynthesis cube.
The researchers used a method by which the average displacement over the breathing cycles was zero. To accelerate reconstruction, curved back projection lines from the motion model were approximated by piecewise linear subsections with a maximal deviation of half a voxel, allowing for real-time surveillance of patients treated with VMAT.
The researchers then conducted image quality analysis. They visually assessed the respiratory artifact reduction and quantified the reduction by fitting a cumulative Gaussian function to profiles along the background-GVT transition in the cranial-caudal projection. Motion compensation considerably reduced artifacts in regions with substantial respiratory induced motion. Tumors were more visible by deblurring the moving tumor and local blurring of the over-projected static ribs.
"Traditionally, IGRT was based on 2D images that often lack soft tissue contrast and are hard to interpret due to the over-projection of anatomy. Therefore 3D image modalities that provide soft tissue contrast, such as megavoltage CT and CBCT, have been introduced," explained co-author Jan-Jakob Sonke, PhD.
"Recently, the acquisition of kilovoltage-CBCT concurrent with VMAT delivery was developed to capture the anatomy during actual treatment. The acquisition time of such 3D images, however, is typically 30 seconds to two minutes and thus they have limited temporal resolution. Digital tomosynthesis is a limited-angle CBCT reconstruction. By changing the angle of the acquisition arc, an optimal compromise can be sought between contrast and temporal resolution."
Additional research to validate the potential of motion-compensated digital tomosynthesis as a surveillance system for delivery of VMAT-based treatment plans is currently underway, Sonke said. The research team plans to evaluate a group of 32 patients with a variety of tumor peak-to-peak amplitudes.
Sonke told medicalphysicsweb that the researchers are working to develop a fast, robust registration method to quantify intrafractional position variability of the time-averaged mean target position. Additionally, they want to identify the peak-to-peak amplitude for which motion-compensated digital tomosynthesis has a clear benefit over conventional digital tomosynthesis, in terms of both image quality and image registration accuracy. They also plan to develop techniques to update the a priori motion model used in the motion-compensated digital tomosynthesis reconstruction, to account for variability in patient-specific motion patterns.
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community website covering fundamental research and emerging technologies in medical imaging and radiation therapy.