Patients undergoing coronary CT angiography (CCTA) no longer have to hold their breath when doing so is challenging for them. According to a new study in European Radiology, CCTA images acquired on a 320-detector-row scanner using a free-breathing technique had similar image quality to those of patients practicing the traditional breath-hold.
An analysis of images acquired in 74 patients showed no significant image quality differences between free-breathing and traditional breath-hold techniques, though the free-breathing scans trended slightly toward higher radiation doses, noted the Korean study team.
"Free-breathing CCTA using 320-detector [multidetector] CT did not show any significant difference in image quality from standard breath-holding CCTA," wrote Dr. Eun-Ju Kang and colleagues from Dong-A University College of Medicine in Busan and Kyungpook National University and Hospital in Daegu (Eur Radiol, 9 November 2012).
CCTA has traditionally been performed with a breath-hold, but some patients cannot do so during CCTA exams because of a number of conditions such as deafness, severe pulmonary disease, lack of cooperativeness, or heart rates that rise during a breath-hold. But 320-detector-row CT, with axial coverage of 16 cm, can perform wide-area nonspiral ECG-gated CCTA during a single R-R interval with 0.175 ms temporal resolution, reducing whole-heart scan times to less than a second and enabling free-breathing CT in patients who need it.
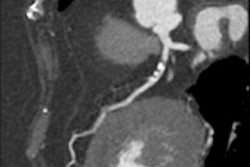
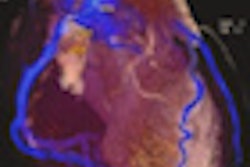
 A 62-year-old man presented for coronary CT angiography (CCTA) due to chest pain. Free-breathing prospective CCTA images show the clearly defined coronary arteries with calcified plaque (arrows) without motion artifacts. All images courtesy of Dr. Eun-Ju Kang.
A 62-year-old man presented for coronary CT angiography (CCTA) due to chest pain. Free-breathing prospective CCTA images show the clearly defined coronary arteries with calcified plaque (arrows) without motion artifacts. All images courtesy of Dr. Eun-Ju Kang.
In addition, previous research shows that motion shift during breathing does not produce more displacement than the beating heart, Kang and colleagues explained.
"According to a report by Mao et al, coronary artery shifting velocity by cardiac pulsation is 22.4-108.6 mm/s," they wrote. "Therefore, the cardiac shifting velocity produced by respiration should be lower than coronary artery shifting velocity by cardiac pulsation in the resting state. We can imagine that the shifting of the coronary artery by respiration is much less than that by cardiac pulsation."
The authors hypothesized that gentle steady breathing during 320-detector-row multidetector CT (MDCT) may not produce additional significant motion artifact; and the study investigated the feasibility of free-breathing CCTA based on image quality and radiation dose.
The study looked at 74 patients who underwent CCTA (24 women, 50 men; mean age, 58 ± 10.9 years, range, 23-76 years) on a 320 detector-row scanner (Aquilion One, Toshiba Medical Systems). Thirty-seven exams were performed during free-breathing, and 37 exams were performed with standard breath-holding. Patients with irregular heart rates or resting rates greater than 75 bpm were excluded. The remaining patients were taught to breathe quietly or perform a breath-hold, depending on the protocol.
After a nonenhanced calcium scoring scan, CCTA exams were performed using 320 x 0.5-mm collimation, 350-ms gantry rotation time, and 175-ms temporal resolution. Tube voltage and current were adjusted to the patient's BMI, with tube voltages of 100-120 kVp and tube currents of 400-550 mA. The patients received 70 mL of nonionic contrast, and beta-blockers if the heart rate was greater than 65 bpm, the authors noted.
Readers examined axial images reconstructed with a slice thickness of 0.5 mm, and a field-of-view adapted to the size of the heart. They evaluated image quality scores for 16 segments of the coronary arteries where one was excellent, two was good, and three was poor, also comparing signal-to-noise ratios (SNR) and contrast-to-noise ratios (CNR), and differences in the radiation dose.
The mean effective dose was 5.9 ± 1.9 mSv for prospective CCTA (n = 11) and 6.5 ± 1.1 mSv for the retrospective CCTA (n = 63), while mean CTDIvol, acquisition length, dose-length product, and effective dose didn't differ significantly between the prospective and retrospective protocols.
The authors found no significant differences in the image quality scores the breath-holding (1.10 ± 0.31) and free-breathing techniques (1.12 ± 0.33; p = 0.443). The SNR and CNR were not significantly different between the two methods. The overall mean effective radiation dose revealed no significant difference between the two methods (p = 0.585).
Mean image background noise was 34.3 ± 6.7 HU, at the aorta, with no significant differences between the two techniques or between retrospective or prospective gating.
Of 963 evaluable segments 1.5 mm and larger, 37 segments were missing because of anatomical variants, and 14 segments were distal to an occluding stenosis, they wrote.
Breath-hold CT and free-breathing CT
|
Image quality comparison shows no significant differences between breath hold and free-breathing techniques.
The principal advantage of 320-detector-row CT being its 16-cm anatomic coverage, "our study was based on this feature of the 320-detector CT system, and the results showed nearly the same image qualities between free-breathing and breath-holding CCTAs," Kang et al wrote. The feasibility of free-breathing CCTA has been previously studied only in children, and the authors said they were not aware of any studies comparing free-breathing to breath-hold techniques, they noted.
The study excluded patients who underwent CCTA with multisegment reconstruction. Although the technique can improve temporal resolution in patients with fast heartbeats, the position of the heart is significantly different over two or three cardiac cycles, producing beat-to-beat artifacts after multisegment reconstruction, they wrote.
Unexpectedly, free-breathing did not require larger CT data acquisition coverage than breath-hold exams, but the detector width cannot be altered in increments less than 2 cm, and less extra coverage may have been needed for free-breathing exams.
"Free breathing CCTA has the possibility of higher radiation dose exposure than breath-holding CCTA, because [it] may require slightly larger scan coverage," Kang wrote in an email to AuntMinnieEurope.com. "So it should be used based on strict indications such as patients who cannot cooperate and hold their breath or whose heart rate increases during breath-holding."
The main limitations of the study are that different patients were studied using different techniques, and that the study population was small, the group stated.
The authors concluded that there were no differences in image quality between free-breathing and breath-hold techniques at 320-detector-row CCTA.
"For patients with difficulties holding their breath or non-negligible apnea-related heart rate variability, free-breathing CCTA during a single heart beat can be an alternative solution for coronary artery evaluation if the heart rate is not elevated (< 75 bpm)," Kang et al concluded.