Everything that's bright on PET/CT scans is not pathological, and everything that's cold on these scans is not benign. This is one of the key points to remember when interpreting images, according to a group of specialists from one of Europe's leading cancer centers.
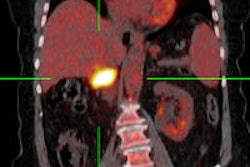
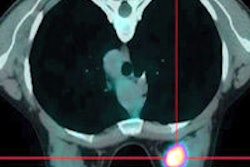
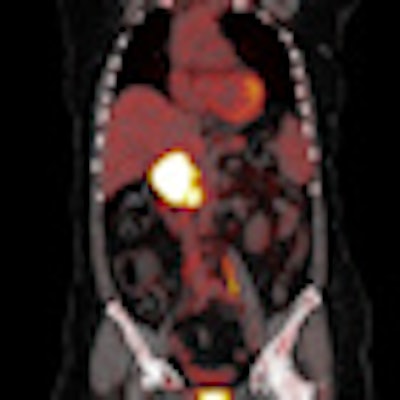
 PET/CT offers significant clinical benefits but has also brought its own potential pitfalls and difficulties in interpretation. Image courtesy of Dr. Osman Ratib, PhD, Geneva, Switzerland.
PET/CT offers significant clinical benefits but has also brought its own potential pitfalls and difficulties in interpretation. Image courtesy of Dr. Osman Ratib, PhD, Geneva, Switzerland.
"Understanding of the technical aspects of PET/CT is vital as these can influence the FDG uptake of the tumor," noted Dr. Uma Viswanathan Nair, clinical fellow for PET/CT at the Christie Hospital National Health Service (NHS) Foundation Trust in Manchester, U.K. "Awareness of normal FDG distribution is crucial in image interpretation."
PET/CT can help greatly in the early detection of increased metabolic activity in diseased tissues, which may appear normal with other imaging modalities, and the technique is used increasingly in patients with malignancies, both as baseline and as part of follow-up, the researcher told attendees at the 2012 U.K. Radiological Conference (UKRC). However, PET/CT scans can pose serious problems for general radiologists involved in multidisciplinary teams, so it's important to bear in mind these pointers:
- Physical distribution of FDG is seen in brown fat, muscles, and soft tissues. It is important not to overcall physiological FDG uptake in the head/neck region and in the bowel as pathological uptake.
- Vigorous exercise in the days just before a PET/CT scan can cause intense uptake in the associated skeletal muscles. Skeletal muscle uptake could also be due to stress-induced muscle tension, and hyperventilation may also induce uptake in the diaphragm. Using insulin to adjust the serum glucose level immediately before injection of F-18-FDG can result in F-18-FDG accumulation in skeletal muscle. Benzodiazepines may be used to decrease paraspinal and posterior cervical muscle uptake in particularly tense patients.
- Normal bone marrow demonstrates minimal generalized uptake. Intermediate to intense FDG-uptake is seen in post-treatment red bone-marrow reactivation.
- Pelvic ureteric uptake may be misinterpreted as nodal activity. In the event of extravasation of contrast, ipsilateral axillary nodes may demonstrate FDG uptake. It is important to be aware of this so that the reporting radiologist can dismiss this uptake as nonpathological, the researchers pointed out.
- Brown fat uptake can result in difficulty in PET/CT interpretation. Brown fat is usually seen in newborns, and the amount of brown fat reduces with age. It provides a "sympathetic response to cold," and this is usually seen in the supraclavicular foss, axilla, around large vessels in the mediastinum and paraspinal, intercostal, perinephric, paracolic, and parahepatic spaces.
- Respiration can result in misregistration of FDG activity.
- False-negative uptake is associated with low cellular malignancies. Some examples of such malignancies are mucinous tumors, bronchoalveolar cell carcinoma, carcinoid, and low-grade lymphoma (e.g., mucosa-associated lymphatic tissue lymphomas).
Other experts have some advice in this area, too.
"Accurate anatomic localization of foci of [F-18-labeled FDG] signifying increased metabolic activity on PET can be difficult or impossible. This is particularly so in the abdomen and pelvis, where there is a lack of reliable identifiable landmarks and variable physiologic FDG uptake," stated Dr. Michael Blake, assistant professor of radiology at Harvard Medical School in the U.S. in a chapter about PET/CT Interpretation in the Elsevier textbook, Abdominal Imaging.
The advent of PET/CT has successfully combined the metabolic information obtained by FDG-PET with the morphologic imaging information of CT, but even though the fusion of the two separate datasets results in more accurate localization of abnormalities and improved overall performance, it has also brought its own potential pitfalls and difficulties in interpretation, he noted.
Furthermore, there are logistic issues of interpretation that still need to be resolved about who should report these studies, he added. In time, there will be more physicians with dual training in both PET and CT, but currently at Massachusetts General and some other academic centers, PET/CT reporting is done as a consensus between the nuclear medicine department as well as the chest and abdominal divisions of the radiology department.