PET/CT is now a useful tool in detecting and restaging recurrent breast cancer, and full use of FDG-PET/CT must be made for follow-up and restaging of patients with the disease, a joint Egyptian and German research team has found.
"Early diagnosis and accurate staging of locoregional and distant recurrence after treatment of breast cancer is decisive for further therapeutic planning," lead researcher Dr. Sally Emad El-Din, from the radiology department at Cairo University Teaching Hospitals, reported at the recent U.K. Radiological Congress (UKRC) in Liverpool. "Combined FDG-PET/CT has been recently introduced as a whole-body imaging modality for examining patients with suspicion of recurrent breast cancer and for accurate staging of metastatic disease."
Her aim was to evaluate retrospectively the clinical implementation of FDG-PET in following up and restaging recurrent breast cancer patients. She reviewed the datasets from 34 women with a history of breast cancer who underwent PET/CT examinations at the Johann Wolfgang Goethe University Hospital in Frankfurt am Main, Germany, between April 2008 and June 2010. Dr. Thomas Vogl, PhD, and Dr. Marc Harth, both from J.W. Goethe University Hospital, were among her co-authors.
The indications of PET/CT were suspected recurrence of breast cancer (44.1% of patients), follow-up in asymptomatic cases (20.6%), whole-body staging in diagnosed cases of recurrence (14.7%), follow-up after local ablative therapy of hepatic metastases (14.7%), and follow-up after treatment of bone metastases (5.9%).
Absence of disease was encountered in 13 out of 34 (38.2%) patients by clinical and imaging follow-up. The PET/CT examination was considered pathological in 21 out of 34 cases (61.8%), the team noted.
The PET/CT interpretations were correct in 31 out of 34 patients (91.2%). Incorrect interpretation occurred in three patients, and there were two false negatives and one false positive. The PET/CT examination had a sensitivity of 90.5% and a specificity of 92.3%. The positive predictive value (PPV) and negative predictive value (NPV) were 95% and 85.7%, respectively.
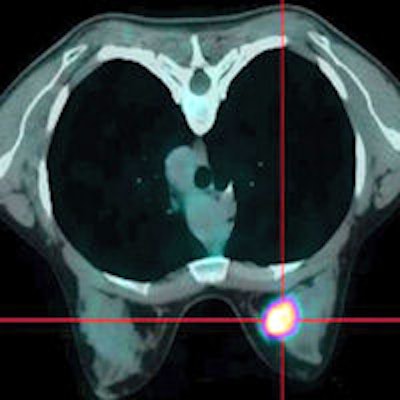
The reason for the false positive was a pulmonary nodule, according to the researchers. The 86-year-old patient had a history of breast cancer 13 years previously. She was referred for the evaluation of new onset of a solitary pulmonary nodule. PET/CT showed increased glucose metabolism -- SUVmax (maximum standardized uptake value) 4.2 -- of the nodule, which was highly suspicious of malignancy. When the follow-up CT examination was performed a month later, the nodule had disappeared and bilateral pleural effusion had developed.
The two false negatives were due to an axillary lymph node metastasis in one patient and suprarenal metastases in the other one.
In five patients with known metastatic disease, PET/CT detected additional unknown metastases in 3 out of 5 women. When there was an increase in metabolism with no morphologic abnormality detected on CT, PET/CT was able to detect bone metastases at an early stage.
PET/CT provides a noninvasive whole-body evaluation in a single examination, she concluded.
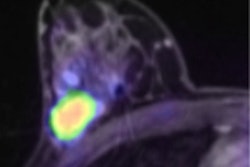
Editor's note: Image on our home page is of a 32-year-old woman with ductal infiltrating adenocarcinoma measuring 18 mm in maximum transverse diameter. Axial fused PET/CT images obtained with patient in prone position. Courtesy of the American Roentgen Ray Society.