The use of cardiac CT for chest pain is evolving toward the use of perfusion CT imaging before intervention, according to a discussion on the triage of patients with suspected coronary artery disease.
In the research setting at least, CT stress perfusion is broadening the range of patients who might be able to rely on CT to avoid more invasive intervention, said Dr. Joachim Wildberger, professor and head of radiology at the University of Maastricht in the Netherlands. In the process, it is working its way from investigational to clinical use.
"Perfusion imaging is certainly the new kid on the block. There have been a number of perfusion imaging papers the last few years so it will hopefully make its way into clinical practice, but honestly it's still quite complicated," Wildberger said at the 2012 International Symposium on Multidetector CT.
Parsing the indications for cardiac CT in chest pain based on the 2010 multisociety appropriate use guidelines (JACC, June 2010, Vol. 56:22 pp. 1864-1894), Wildberger noted that CT is an important modality for life-threatening conditions, including:
- Acute pulmonary embolism
- Acute aortic pathology
- Acute coronary syndrome
- Esophageal rupture
- Pericardial tamponade
- Tension pneumothorax
However, life-threatening myocardial infarction (MI) isn't one of them, he said. MI patients should undergo quantitative coronary angiography instead because it offers a chance of immediate treatment according to the 2010 appropriate use criteria, he explained.
"We know that time is muscle and we actually have reached an irreversible state with myocardial infarction," he said. For cardiac CT it makes more sense to focus on reversible conditions, as well as potentially life-threatening conditions.
"And in that we're much more interested in the exclusion of disease -- discharging the right patients and that's why the triple rule-out came up several years ago," Wildberger said. "The ultimate goal is to rule out patients with a low-to-intermediate pretest likelihood of coronary artery disease, accurately and noninvasively."
- Thus, for patients with acute symptoms and suspicion of acute coronary syndrome (normal ECG and cardiac biomarkers or nondiagnostic ECG or equivocal biomarkers) CT is appropriate for patients with low or intermediate pretest probability of coronary artery disease.
- For acute symptomatic patients with a high pretest probability, the indication for CT is uncertain, as it is for individuals with persistent ECG ST segment elevation following exclusion of myocardial infarction or triple rule-out.
- Patients with a nonacute presentation would generally have an ECG and probably an exercise treadmill test, Wildberger said. Those who can exercise can be placed at intermediate probability of disease and scanned; if they can't exercise, barriers to CT become less important and the patient can be scanned with low appropriateness, he said.
That's where the cardiac CT diagnostic algorithm is heading -- toward broader use, Wildberger said. When there is acute chest pain and acute coronary artery disease is anywhere in the list of differential diagnoses, triage is the key to success. Before the patient goes into the scanner, clinicians should have a good history of physical exam, ECG, lab tests, and risk stratification for the patient, he said.
Chest pain patients with ST elevation myocardial infarction (STEMI) or non-ST elevation myocardial infarction (NSTEMI) should go straight to percutaneous coronary intervention, while those with negative or nonspecific findings can be considered for CT angiography assessment, for which referral is becoming less restrictive. Why are the barriers falling?
In the past "the dose penalty was a major concern but it's not that striking anymore," Wildberger said. "When you apply this type of protocol on a second-generation dual-source CT scanner, you will end up with a dose of approx 2-3 mSv which is reasonable using the FLASH (Siemens Healthcare) technique," he said.
CT might demonstrate a mild or moderate stenosis, and these patients can probably be discharged safely, while those found to have significant coronary artery stenosis can be referred for percutaneous coronary intervention, he said.
"However, there's a reasonable number of patients who will have functional stenosis, and in these patients functional testing will probably be needed in order to make a clear diagnosis [and determine] whether they are going for medication or have to be admitted to the hospital" for an interventional procedure, Wildberger said.
"So we are actually pushing the envelope forward in the direction of stress perfusion," he said.
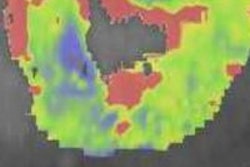
Perfusion CT been performed as far back as 2001 on a four-detector scanner, which was able to show hypovascular structures in the heart muscle stemming from a coronary artery obstruction, he said.
"We did some studies in first-pass perfusion and were able to show that this is a finding that can also be seen on MR and on histologic specimens as well," he said. Color-coded for first-pass perfusion or late enhancement, perfusion CT reliably depicts areas at risk.
Perfusion is likely headed into routine clinical practice, even though the scan is still somewhat complicated to perform, Wildberger said.
In August, researchers at the European Society of Cardiology Congress in Munich presented the first larger-scale study of perfusion CT. Performed on 381 patients on a 320-detector-row wide-area scanner, the addition of a perfusion scan to coronary CT angiography substantially boosted the diagnostic accuracy, more accurately predicting the need for invasive intervention.