The increasing use of CT in emergency medicine means that radiologists have become significant members of the clinical team making key decisions about the therapeutic process, according to a Czech expert on trauma imaging.
The great strength of multidetector-row CT (MDCT) is its high speed and high geometric resolution in any plane, noted Dr. Hynek Mirka, PhD, deputy head of research and development in the department of imaging methods at Charles University and University Hospital in Pilsen, Czech Republic. It makes it possible to view large parts of the body with minimal motion artifacts and to create accurate multiplanar and 3D reformations, which boosts the accuracy of the diagnosis significantly. Because of these advantages, MDCT has become the first-choice method in high-energy traumas.
 Chest CT, coronal reformation in the lung window. Left-sided tension pneumothorax, extensive contusion of the left lung with lacerations and subcutaneous emphysema of the left hemithorax. All images courtesy of Dr. Hynek Mirka, PhD.
Chest CT, coronal reformation in the lung window. Left-sided tension pneumothorax, extensive contusion of the left lung with lacerations and subcutaneous emphysema of the left hemithorax. All images courtesy of Dr. Hynek Mirka, PhD."Imaging methods are an integral part of the diagnostic algorithm in chest injuries. MDCT is its main component. It shows traumatic changes quickly, accurately, and clearly, and allows their classification," he wrote in an article published online on 4 August by Insights into Imaging. Chest traumas are a significant cause of mortality and morbidity, especially in the younger population. Diagnostic imaging plays a key role in their management."
In the article, Mirka and colleagues summarize the position of MDCT in the diagnostic algorithm of chest injuries, technical aspects of the examination, and imaging findings in traumas of the individual chest compartments. They explain how detailed information can be acquired in a short acquisition time, and multiplanar and 3D reformatting make the diagnosis significantly more accurate.
Chest injuries occur in about 20% of all trauma patients. In up to 80% of cases, they are associated with injuries of other body parts such as the head (69%), abdomen and pelvis (43%), and extremities (52%), the authors pointed out. These injuries usually occur in car crashes, falls from heights, sports injuries, and violent acts. The most affected compartments include the chest wall (> 50%), pleura (50%), and lungs (30% to 70%), while traumas of the airways (2.8% to 5.4%), diaphragm (0.4% to 1.5%), large vessels (1.1% to 2.2%), and heart (10%) are rare but often very severe, they stated.
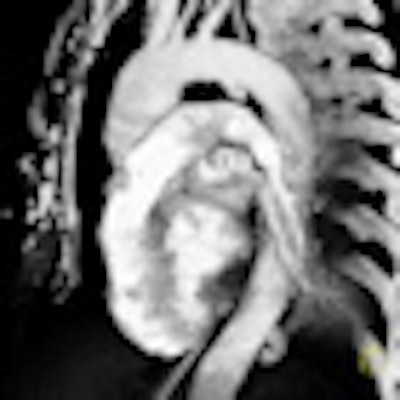
 Postcontrast chest CT, black-and-white volume rendering reconstruction, sagittal view. Aortic isthmus laceration -- pseudoaneurysm in a typical location.
Postcontrast chest CT, black-and-white volume rendering reconstruction, sagittal view. Aortic isthmus laceration -- pseudoaneurysm in a typical location."According to the underlying cause, the injuries are classified as blunt (90%) and penetrating (10%) injuries. Blunt injury is caused by three basic mechanisms, which are often combined. These are a direct impact, compression, and deceleration. Direct impact on the chest causes a localized injury of the chest wall at the point of contact," they noted. "When exposed to major forces, the energy can affect the deeper structures located in their trajectory, such as lungs, heart, blood vessels, mediastinum, liver, or spleen. Compression causes pressing of the organs against the spine or chest wall and their contusion or rupture. The pulmonary parenchyma, pleura, diaphragm, and tracheobronchial tree are often affected."
Clinical symptoms of chest injuries are diverse and often do not correlate with their severity, and this explains why imaging is among the first procedures performed after admission to hospital, they added. Chest radiography and ultrasound can, especially in unstable patients, provide important information about the presence of serious injuries requiring an emergency intervention, such as tension pneumothorax, large hemothorax, hemopericardium, hemoperitoneum, and injuries of the abdominal organs under the diaphragm.
"These methods are less sensitive for some types of trauma, and therefore, especially in high-energy injuries they cannot be considered as conclusive," the authors wrote. "Chest radiography is performed in severe injuries in supine position, which further reduces its contribution. Detection of a contusion and laceration of the pulmonary parenchyma, but also a smaller hemothorax and pneumothorax, is also an issue. It is also very unreliable in detecting injuries of the heart and great vessels. In addition to low sensitivity in certain types of traumas, its low specificity is a problem."
Chest wall injuries are very common, and fractures reflect the intensity and direction of forces during trauma, but the extent of a chest wall injury does not have to correlate with the injuries of the intrathoracic organs, they added. This is evident, especially in children and young adults with a flexible skeleton in whom severe visceral traumas may occur despite there being no fractures.
Injury to the lung parenchyma includes pulmonary contusion, laceration, torsion, and herniation. These conditions can be complicated by atelectasis, aspiration pneumonia, or acute respiratory distress syndrome. Lung trauma is seldom a reason for surgical treatment, according to the authors. This is indicated in cases of injury of the major blood vessels, signs of active bleeding, large hematomas, or hemodynamic instability in the context of pulmonary involvement.
"Due to the fact that our department systematically deals with MDCT of the trauma, further work on this subject can be expected in the future," Mirka noted in an email to AuntMinnieEurope.com.


















