The use of chest tomosynthesis with a digital radiography (DR) system enabled radiologists to characterize pulmonary lesions, circumventing the need for further diagnostic workup of patients with CT, according to a study by Italian researchers. They presented their findings in a poster presentation at the RSNA 2011 meeting in Chicago.
The group has been investigating whether DR tomosynthesis could eliminate the use of CT in some patients with suspicious pulmonary lesions by enabling lesions to be characterized as malignant or benign with DR alone. By creating 3D reconstructions from a series of 2D x-ray slices, tomosynthesis solves the problem of overlapping structures that frequently confounds traditional x-ray.
"Since the chest is a 3D structure, the problem with chest x-ray is every plane is compressed through the image," said Dr. Emilio Quaia and Dr. Elisa Baratella from the department of radiology at University of Trieste. "Tomosynthesis allows you to analyze every single plane of the volume, avoiding the overlap with the adjacent structure, including vessel, rib, and heart structure, which can sometimes create pseudolesions."
Normally, a patient is referred for a chest x-ray and then followed up with chest CT. However, in this study, 339 patients underwent chest x-ray and then digital tomosynthesis (Definium 8000, GE Healthcare). Two independent readers rated the lesions on a five-point scale, with 1 meaning definitely or probably a benign or calcified extrapulmonary lesion or pseudolesion, and 5 meaning probably or definitely a noncalcified pulmonary lesion.
Based on the reader's score of digital tomosynthesis images, the patients could be sent for chest CT. In patients who did not receive chest CT, the digital tomosynthesis findings had to be confirmed six to 12 months later.
Digital tomosynthesis identified a total of 173 thoracic lesions, of which 125 were pulmonary and 48 were extrapulmonary. In the remaining 166 patients, digital tomosynthesis did not confirm any lesions that were considered to be pseudolesions.
Chest x-ray and tomosynthesis differed in terms of accuracy (43% versus 90% for reader 1 and 49% versus 92% for reader 2). Only 81 out of 339 patients underwent CT, since digital tomosynthesis confirmed the presence of true pulmonary noncalcified lesions.
 |
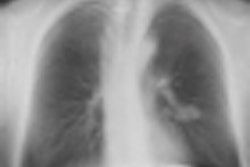
| Chest digital tomosynthesis detected lung calcifications (left) as verified by CT (right). Images courtesy of Dr. Emilio Quaia. |
The study highlights several benefits to using digital tomosynthesis rather than CT for working up some patients, Quaia said.
"The first advantage is to avoid CT workload because three-fourths of the patients are excluded from CT," Quaia said. The second advantage is dose -- digital tomosynthesis dose was 0.2 mSv, while CT dose ranged from 1 mSv to 8 mSv.
Lastly, tomosynthesis cut patient waiting times from three weeks to five days because some patients may receive tomosynthesis right away or within a few days, whereas it can take weeks to schedule a CT exam at the researchers' institutions.
The Italian team's results parallel another study presented at RSNA 2011 by Swedish researchers, who found that they were able to use chest tomosynthesis alone in many patients to rule out pathology without the need for CT.
"Tomosynthesis is a troubleshooting technique for the reasons why the patient [is being] referred but sometimes there are additional lesions that cannot be detected with traditional chest x-ray," Quaia said.