New research conducted in the Irish Republic has highlighted the dangers of hurling, the world's oldest field game. In spite of more protective measures, musculoskeletal injuries remain common among young adults and are encountered frequently by the country's radiologists.
"Approximately 250 persons attend the emergency department per year with various hurling-related injuries, mostly young adults, particularly during the peak season and school matches. Hand, wrist, and upper limb injuries are the commonest," noted Dr. Nagabathula Ramesh, from the department of radiology at Midland Regional Hospital in Portlaoise, Republic of Ireland.
 In hurling, the stick, or "hurley," is curved outward at the end, to provide the striking surface, and the ball, or "sliotar," is similar in size to a hockey ball but has raised ridges. All images courtesy of Dr. Nagabathula Ramesh.
In hurling, the stick, or "hurley," is curved outward at the end, to provide the striking surface, and the ball, or "sliotar," is similar in size to a hockey ball but has raised ridges. All images courtesy of Dr. Nagabathula Ramesh.In hurling, one of Ireland's favorite games, movement is fast; the ball moves at tremendous speeds, and tackling is allowed, but not to the extent seen in rugby, all of which can lead to serious sports injuries, he told attendees at the 2014 meeting of the European Society of Musculoskeletal Radiology (ESSR), held in Riga, Latvia.
The most common cause of injuries is when a player is tackled by another player, and the injuries range from simple bruising and abrasions to severe dislocations and multiple system trauma. Upper extremity trauma tends to be more common in hurling, particularly the hand and the wrist, while orbital and facial are common in both types of sports, Ramesh explained.
 Male, 20, sustained fracture to base of the proximal phalanx of the index finger during training.
Male, 20, sustained fracture to base of the proximal phalanx of the index finger during training.Hurling is played on a pitch that can be up to 145 m long and 90 m wide. The stick, or "hurley," is curved outward at the end, to provide the striking surface, and the ball, or "sliotar," is similar in size to a hockey ball but has raised ridges. The goalposts are similar to those used on a rugby pitch, with the crossbar lower than in rugby and slightly higher than a soccer one. A player can strike the ball on the ground or in the air, and unlike hockey, you may pick up the ball with your hurley and carry it for not more than four steps in the hand, he added.
As of 2010, all players must wear a helmet, and may wear other protection such as shin guards and/or a special kind of glove. This has had a positive impact, as shown by research published last year by the British Journal of Sports Medicine (January 2014, Vol. 48:2, pp. 147-150). However, often young adults and school children have inadequate protection while playing the game.
 Male, 40, sustained nasal bone fracture during a league match. He was not wearing a protective helmet.
Male, 40, sustained nasal bone fracture during a league match. He was not wearing a protective helmet.At the ESSR meeting in Riga, Ramesh also presented research about sports-related injuries in cricket. The repetitive nature of the game, as well as the need often to be out on the field of play for long periods, predispose cricketers to a wide range of injuries, and injury can occur during any phase of the game (bowling, wicket-keeping, batting, or fielding) and can involve any part of the body.
"Although strictly a noncontact sport, injuries in cricket can result in a number of ways," he elaborated. "A direct blow from a cricket ball during delivery or fielding may result in fractures, bruising, or a fielder may fall or collide with other fielders. Cricketers also suffer from a range of overuse injuries associated with all aspects of the game including running, throwing, batting, and bowling; the latter was found to be the most common. Injuries were found to be more common in children and in lower-league matches (80%). Lower limb and back injuries accounted for more than 90% of the injuries."

Hamstring strains and injuries are common in fast bowlers. Injuries of the hands/fingers such as avulsion fractures and dislocations are usually a result from a player catching the ball and are common. Rotator cuff injuries are often seen in fast bowlers and fielders, with labrum injuries commonly seen in fielders.
Lower back pain is usually associated with fast bowlers due to extension and rotation forces, including disk herniation and spondylolysis. Mechanical factors play an important role in the etiology of degenerative processes and injuries to the lumbar spine, and this is particularly so in fast bowling -- a player must absorb vertical and horizontal components of the ground reaction force that are approximately five and two times body weight at front-foot and rear-foot impact respectively, according to Ramesh.
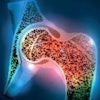
 Male, 33, sustained anterior inferior dislocation of the humeral head during inter-club match.
Male, 33, sustained anterior inferior dislocation of the humeral head during inter-club match.Additional forces are transmitted to the spine through the lower limb, while additional forces at the lumbo-sacral junction are caused by trunk hyperextension, lateral flexion, and twisting during the delivery stride. Outfield players (fielders) and bowlers do not wear any protective equipment, except close-in fielders, who wear helmets. The wicket keeper usually wears a helmet, gloves, and pads. The batsman is the best protected of them with helmet, gloves, and leg and forearm pads.
"One of the best ways of avoiding injury is to ensure full warm-up, involving 10-15 minutes of cardiovascular exercise, increase the body and muscle temperature, and improve muscle elasticity. This is followed by stretching-active and static-exercises," he concluded. "Throwing and batting practice are needed to prepare mentally. Adequate protection at all levels of the league players need to be encouraged."