When it comes to breast MRI, reporting benefits more from using a diagnostic algorithm rather than expert experience in a clinical, problem-solving setting, Austrian researchers have asserted in an article posted on 19 July by European Radiology.
The Kaiser score, which provides a clinical decision algorithm for structured reporting, helps radiology trainees to reach an expert level in breast MRI reporting and to even outperform experienced radiologists using MR BI-RADS without further formal guidance, according to first author Dr. Nina Pötsch and colleagues at the Medical University of Vienna.
These results support that reporting breast MRI benefits more from using a diagnostic algorithm rather than expert experience, they pointed out.
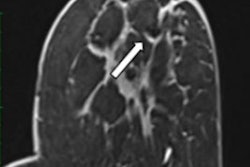
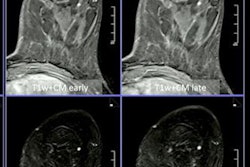
 B2 lesion rated BI-RADS 4/5 by experts and benign using the Kaiser score. T2 turbo-spin echo (A), early (C) and late (E) postcontrast T1 with fat suppression, as well as corresponding magnifications of the right breast (B, D, F). This lesion was rated as MR BI-RADS 4 or 5 by the experts. Applying the Kaiser score to this mass lesion without spiculations, persistent enhancement, and irregular margins gives a Kaiser score of 3, which is a benign result corresponding to a BI-RADS 2/3. Histologic verification showed tumor-free mammary parenchyma with low-grade pseudoangiomatous stromal changes, B2. (All figures courtesy of Dr. Nina Pötsch and European Radiology)
B2 lesion rated BI-RADS 4/5 by experts and benign using the Kaiser score. T2 turbo-spin echo (A), early (C) and late (E) postcontrast T1 with fat suppression, as well as corresponding magnifications of the right breast (B, D, F). This lesion was rated as MR BI-RADS 4 or 5 by the experts. Applying the Kaiser score to this mass lesion without spiculations, persistent enhancement, and irregular margins gives a Kaiser score of 3, which is a benign result corresponding to a BI-RADS 2/3. Histologic verification showed tumor-free mammary parenchyma with low-grade pseudoangiomatous stromal changes, B2. (All figures courtesy of Dr. Nina Pötsch and European Radiology)The aim of the researchers was to evaluate the diagnostic performance of untrained residents using the Kaiser Score compared with offsite radiologists experienced in breast imaging using only MR BI-RADS. Three offsite, board-certified radiologists experienced in breast imaging interpreted MRI scans according to the MR BI-RADS scale.
The same studies were read by three residents in radiology without prior training in breast imaging using the Kaiser score. All readers were blinded to clinical information, and histology was used as the gold standard.
A total of 80 women (median age, 52 years) with 93 lesions (32 benign, 61 malignant) were included in the study. The individual within-group performance of the three expert readers (area under curve [AUC], 0.723-0.742), as well as the three residents, was equal (AUC, 0.842-0.928). But the rating of each resident using the Kaiser score significantly outperformed the experts' ratings using the MR BI-RADS scale.
Is CEM as good as breast MRI?
The idea for this new study came from the Vienna group's 2020 article posted in the Journal of MRI.
"We published findings in line with the repeated narrative that 'contrast-enhanced mammography (CEM) is practically as good as breast MRI' -- results that seriously surprised me," study co-author Dr. Pascal Baltzer told AuntMinnieEurope.com.
Because offsite readers were used in the 2020 study, the authors had no involvement in the image analysis, but they knew the cases because they took part in patient recruitment and organizational aspects.
"I wondered about the very low specificity achieved by the off-site readers for breast MRI. How could that be in a study that was due to the inclusion criteria rather biased towards lager and thus more simple to assess lesions? How could an expert call a 2 cm pathognomonic fibroadenoma suspicious?" Baltzer said.
"A nagging thought came up: Can it really be true that they just recalled enhancing lesions as abnormality?" Baltzer continued.
The Kaiser score guides radiologists in three steps through the BI-RADS criteria and ends up with a diagnosis, and by this, it forces readers to systematically assess these criteria and also gives weight to ambiguous criteria, he noted.
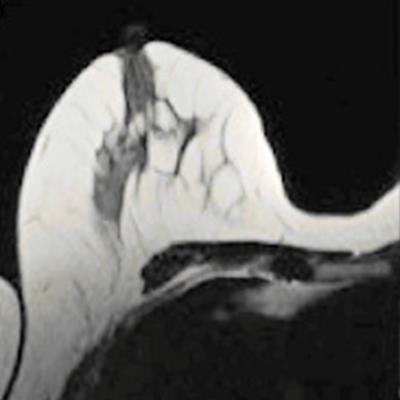
 Fibroadenoma rated BI-RADS 4/5 by experts and benign using the Kaiser score. T2 turbo-spin echo (A), early (C), and late (E) postcontrast T1 with fat suppression, as well as corresponding magnifications of the left breast (B, D, F). This lesion was rated as MR BI-RADS 4 or 5 by the experts. Applying the Kaiser score to this mass lesion without spiculations, plateau enhancement, and circumscribed margins gives a Kaiser score of 2, which is a benign result corresponding to a BI-RADS 2/3. Histologic verification showed a fibroadenoma, B2.
Fibroadenoma rated BI-RADS 4/5 by experts and benign using the Kaiser score. T2 turbo-spin echo (A), early (C), and late (E) postcontrast T1 with fat suppression, as well as corresponding magnifications of the left breast (B, D, F). This lesion was rated as MR BI-RADS 4 or 5 by the experts. Applying the Kaiser score to this mass lesion without spiculations, plateau enhancement, and circumscribed margins gives a Kaiser score of 2, which is a benign result corresponding to a BI-RADS 2/3. Histologic verification showed a fibroadenoma, B2."How can an expert call a type 1 enhancing circumscribed lesion suspicious? Well, only if you apply the logic of conventional breast imaging, i.e., mammography and ultrasound," he said. "Due to the lack of physiological information provided by these methods, you can never categorize a lesion as definitely benign or malignant by imaging and have to recall them in case of doubt."
This, however, is not in line with current knowledge about breast MRI -- e.g., the Kaiser score has definite rule-in and rule-out criteria that practically do not require bioptic verification to confirm the diagnosis. Biopsy would only be required for immunohistochemical subtyping to determine the best suited treatment.
"All this is remarkable: breast MRI is already recognized as a very powerful tool in the breast imager's portfolio even though its interpretation could be easily and remarkably improved by using the Kaiser score. I am therefore very much looking forward to seeing the Kaiser score integrated into BI-RADS," he concluded.