While surgery has long been the cornerstone of the exploration and treatment of the patient with penetrating trauma, imaging today occupies a central place in the management of the trauma patient.
Imaging has multiple roles: It allows the indication, or not, of surgical exploration in most cases -- presence of a pneumoperitoneum suggesting a digestive perforation, solution of digestive parietal continuity, solid organ lesion, arterial bleeding (which may require interventional radiology management), and hemopneumothorax. Imaging also makes it possible to carry out a ballistic assessment. This is particularly the case for deep penetrating injuries (large caliber knives, handguns) and/or multiple (multiple or fragmented bullet holes).
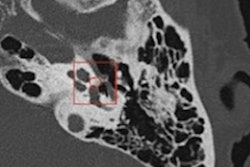
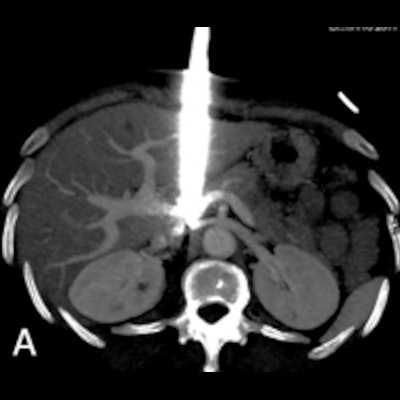
 Two cases that underline the importance of CT examinations in ballistic assessment of trauma. A: Stab trauma coming in close contact with the inferior vena cava. multiple gunshot trauma (B). All images courtesy of the Drs. Mathieu Di Bisceglie, Kathia Chaumoître, and JFR e-Quotidien.
Two cases that underline the importance of CT examinations in ballistic assessment of trauma. A: Stab trauma coming in close contact with the inferior vena cava. multiple gunshot trauma (B). All images courtesy of the Drs. Mathieu Di Bisceglie, Kathia Chaumoître, and JFR e-Quotidien.In nonstable patients, first-line emergency imaging exams -- chest x-ray, pleuropulmonary ultrasound, focused assessment with sonography for trauma (FAST) echo -- are now most often performed by the resuscitation team. Imaging should not cause a delay in the surgical management of the patient.
In stable patients -- stabilized after intensive care, or secondarily stabilized after emergency surgery -- the most exhaustive and rapid additional imaging possible will be offered.
CT's applications
The reference imaging modality is CT. With negative and positive predictive values greater than 80% or even 90% for a serious underlying thoracic or abdominal lesion, CT will make it possible to direct the management of the patient in an emergency and decide on conservative management or surgical/interventional treatment.
The usual diagnostic protocol should include arterial acquisition of the thorax, abdomen, and pelvis, followed by venous acquisition of the abdomen and pelvis. For "simple" penetrating traumas (knives in particular), cases in which the lesional mechanism is known, there are no deceleration lesions, and ballistics for the lesions are suggested by the clinic (visible entry point, possible exit point in the event of a gunshot wound), a more targeted CT scan could be considered.
A late urinary acquisition time (7 minutes) may be achieved in the event of retroperitoneal or pelvic trauma to look for damage to the urinary tract. While the place of spontaneous contrast abdominopelvic imaging is still debated, recent articles suggest that it does not increase diagnostic performance, while increasing the dose delivered to the patient.
The management of the patient presenting with penetrating trauma must be done in a multidisciplinary and collaborative way. The emergency or resuscitation team taking charge of the patient must make an initial assessment (hemodynamics, lesion mechanism, and possible ballistics) adapted to the context of the emergency, and this must be sent to the radiology team, or, if necessary, to the surgical team in the case of an unstable patient after adequate resuscitation measures.
Using these collected data, the radiologist will decide on the appropriate CT acquisition protocol and will transmit interpretation as quickly as possible, most often verbally, about the obvious lesions that require urgent therapeutic management. This is followed by a written report highlighting the trauma elements to be managed and/or monitored as well as other pathological features linked or not to the trauma. The radiologist will communicate this information first to the resuscitation team and then also to the specialized surgical team, if necessary.
The important place of interventional radiology, alone or with surgery, in the therapeutic management of the trauma patient, must be noted, in particular in the context of arterial vascular lesions requiring emergency embolization.
Finally, CT imaging, with its availability in emergency and its diagnostic performance, has a vital role in the management of the patient, namely by determining the appropriate conservative or surgical treatment, or interventional radiology.
Dr. Mathieu Di Bisceglie and Prof. Kathia Chaumoître are radiologists at North Hospital, Aix Marseille University, France. They participated in a JFR session on abdominal emergencies from children to adults, held at 3:45 p.m. on 8 Friday, October 2021 (online session, Channel 4).
Editor's note: This is an edited version of a translation of an article published in French online by the daily newspaper, e-Quotidien, of Journées Francophones de Radiologie (JFR). Translation by Frances Rylands-Monk. To read the original version, go to the JFR website.