Contrast-enhanced ultrasound scans revealed patterns in the lung not typically associated with pneumonia in three Italian patients with COVID-19, according to a report published on 12 May in the Journal of Ultrasound in Medicine.
The three male patients in the study were all admitted to a hospital in Italy with laboratory-confirmed COVID-19 and pneumonia-like symptoms. However, when doctors performed contrast-enhanced ultrasound scans on the patients, they found large perfusion defects in a pattern not typical of pneumonia or lung collapse.
"Our and other observations suggest that there also may be an ulterior pattern of COVID-19 lung involvement in which the consolidations do not represent atelectasis or easily recruitable areas but tissue with large perfusion defects," wrote the team of Italian authors, led by Dr. Gino Soldati from the ultrasound unit at Valle del Serchio General Hospital in Lucca, Italy. "This possibility could be important for managing the ventilatory support of patients with respiratory failure."
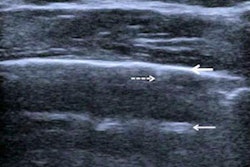
The three patients in the study all underwent radiographic and chest ultrasound examinations within three hours of admission. The ultrasound findings were as expected for patients with COVID-19, including B-lines that were often grouped and confluent in areas of white lung.
However, the three patients also had echographic parenchymal consolidations at the bases and more than one nonbasal subpleural consolidation, less than 2 cm in diameter, with a wedge-shaped or angular appearance.
The subpleural consolidations, combined with high D-dimer values and the inability to perform chest CT, led the doctors to perform contrast-enhanced ultrasound scans. Notable findings included the following:
- Abnormal early arterial enhancement in the first nine seconds following administration. The effect was partial in nature, often not uniform, and displayed no evidence of pulmonary arteries in a segmentary arrangement.
- Incomplete enhancement of major consolidations, especially in the pulmonary cortex.
- Sharp boundaries between perfused and nonperfused areas.
- No enhancement of consolidations less than 2 cm. Instead, the consolidations behaved as ischemic or infarct regions.
"Although some features of COVID-19 resemble those described for the usual viral pneumonia, some morphologic aspects of the lung involvement question the real nature of the consolidative lesions," the authors wrote.
The authors hypothesized that the lung damage they saw could be the result of inflammation from proinflammatory macrophages, granulocytes, and cytokines.
"The cytokine storm causes severe capillary damage and organ dysfunction," the authors wrote. "In the lung, diffuse alveolar damage, hyaline membrane formation, interstitial infiltration of inflammatory cells, fibrin exudate, and fibrotic changes were observed."
Fortunately, the three patients in the study never required invasive respiratory support, and all were discharged 10-12 days after admission. And although more confirmatory research is needed, the contrast-enhanced ultrasound scans could lead doctors to rethink their approach to COVID-19 for some patients, including potentially implementing immunomodulatory therapy for the cytokine storm.
"Our findings may have importance in the pathogenetic interpretation of the consolidations in COVID-19 and consequently, in the ventilatory and medical treatment of patients with COVID-19," the authors wrote.