Imaging can play a central role in the management of gout, one of the most common inflammatory arthropathies in adults and the most common arthritis in men, according to a presentation at the annual scientific meeting (ASM) of the Royal Australian and New Zealand College of Radiologists (RANZCR).
Gout is hallmarked by the deposition of monosodium urate (MSU) crystals in joint spaces and tissue. Once referred to as the “disease of kings and king of diseases,” it has become increasingly common due to the advent of many other chronic comorbidities such as obesity, hyperlipidemia, renal disease, and hypertension, Dr. Roland Zhang, radiology registrar at Gosford Hospital, Gosford, New South Wales, Australia, explained in a poster.
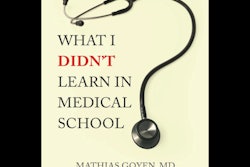
 Diffuse juxta-articular erosions with overhanging edges and preserved joint spaces. Most marked at the first metatarsophalangeal joint (MTPJ) and ulnar styloid. All figures courtesy of Dr. Roland Zhang and presented at RANZCR 2025 ASM.
Diffuse juxta-articular erosions with overhanging edges and preserved joint spaces. Most marked at the first metatarsophalangeal joint (MTPJ) and ulnar styloid. All figures courtesy of Dr. Roland Zhang and presented at RANZCR 2025 ASM.
Gout is the most prevalent inflammatory arthritis in men and one of the most common chronic inflammatory arthropathies in Western Europe, North America, and Australasia. It arises from the supersaturation of body tissues with urate in and around joints, which presents in excruciatingly painful acute attacks, Zhang explained.
The author’s aim was to boost understanding of the presentation, pathophysiology, and radiological appearances of gout, especially in uncommon locations.
 Similar findings of tophaceous gout in typical locations, such as the first MTPJ.
Similar findings of tophaceous gout in typical locations, such as the first MTPJ.
The exhibit described the case of a 59-year-old man who presented to the emergency department after normal working hours with severe pain throughout his body. Examination showed diffuse tophaceous gout in the hands and feet, as well as bilateral lower limb edema and paresthesia. Bedside Doppler ultrasound showed a left common femoral vein thrombus, whilst an echocardiogram showed a dilated aortic root. A double rule-out CT pulmonary angiogram (CTPA) and aortogram was organized.
“On the CTPA and aortogram, several large calcified masses arising from the lower lumbar spine were seen almost completely effacing the L3/4 and L4/5 facet joints and causing moderate-severe spinal canal stenosis,” Zhang pointed out.
Incidental note was made of widespread destructive arthropathy and multiple calcified perivertebral masses in the lower lumbar spine, and a possible bone or soft-tissue-based malignancy causing nerve compression was raised by the medical staff. Imaging was reviewed with radiology. These changes were also found in the bilateral sternoclavicular, glenohumeral, and thoracic costovertebral joints. Prior x-rays were examined, and these changes were determined to be most likely due to tophaceous gout.
 Soft tissue window of a tophus centred in the L2 lamina extending into the neural foramen.
Soft tissue window of a tophus centred in the L2 lamina extending into the neural foramen.
“Hyperuricemia is essential for the development of gout; however, it is not the sole determinant,” the author noted. “Due to the absence of uricase in humans, uric acid is not metabolized into the water-soluble allantoin; hence, urate (a product of purine metabolism) can only be removed through the urinary or gastrointestinal systems. Accumulation of purines results in saturation of urate, which leads to supersaturation and crystallization.”
Gout tends to occur in discrete stages of asymptomatic hyperuricemia, acute gout attack, intercritical gout (where urate deposition persists despite lack of symptoms), chronic tophaceous gout, and gouty nephropathy, Zhang continued.
 Coronal bone window of the neck demonstrates destructive arthropathy of the bilateral sternoclavicular joints with surrounding partially calcified soft tissue masses in keeping with tophi.
Coronal bone window of the neck demonstrates destructive arthropathy of the bilateral sternoclavicular joints with surrounding partially calcified soft tissue masses in keeping with tophi.
Abnormalities on plain x-ray may not be visible for up to eight years, and only reversible clinical features may be apparent during acute attacks, but evidence of destructive arthropathy can be seen early on MRI, according to the author. Classic radiological features of gout are “punched-out” or “rat-bite” lytic lesions, overhanging sclerotic margins, and absence of periarticular osteopenia.
“As the saying goes, common things are common; hence, in the right clinical setting, it is important to consider it as a cause for arthritic changes or calcific soft tissue masses even in unusual locations to avoid unnecessary further investigation,” the author concluded.
The full RANZCR ASM e-poster is available on the EPOS site.