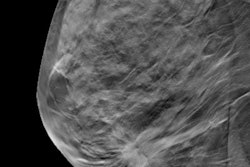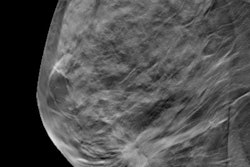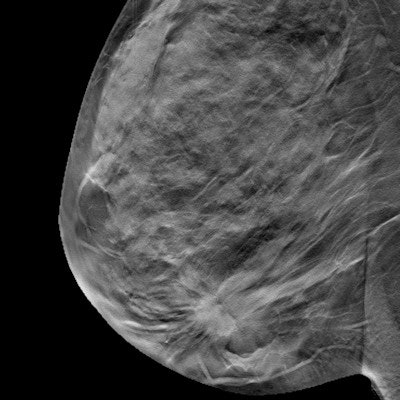
Researchers from Norway have again confirmed that digital breast tomosynthesis (DBT) finds more cancers in most breast density and patient age groups compared with digital mammography -- especially cancers presenting as spiculated masses or architectural distortions, according to a study published online on 13 August in Radiology.
The group also discovered that DBT produced fewer false-positive findings across age and density categories than digital mammography, except in extremely dense breasts.
The results further confirm DBT's place in the breast cancer screening arsenal, particularly for women with dense breasts, wrote a team led by Dr. Bjørn Østerås of Oslo University Hospital.
"The results of our study show that adding DBT to digital mammography in screening yields more cancers in women of all density categories ... and age groups," the group wrote.
Østerås and colleagues compared true- and false-positive interpretations in digital mammography versus DBT according to volumetric breast density, patient age, and mammographic findings, using data from 24,301 women who participated in the Oslo Tomosynthesis Screening Trial between November 2010 and December 2012.
The women underwent digital mammography and DBT, with independent double reading for both; their breast density was evaluated using automatic volumetric software. Østerås' group tracked differences between the two modalities in true-positive rates, false-positive rates, and mammographic findings.
The researchers found that DBT had a higher true-positive rate than digital mammography for most breast density and patient age groups, due to the higher number of spiculated masses and architectural distortions identified on DBT.
| Performance of DBT for breast screening | ||||
| Patient characteristic | Digital mammography only (No. of cancers detected) | Digital mammography plus DBT (No. of cancers detected) | Percentage difference | p-value |
| All women | 177 | 230 | 22.7% | < 0.001 |
| Density | ||||
| Category 1 | 15 | 17 | 13% | 0.50 |
| Category 2 | 79 | 105 | 33% | < 0.001 |
| Category 3 | 64 | 83 | 30% | < 0.001 |
| Category 4 | 18 | 23 | 28% | 0.06 |
| Age | ||||
| 50-54 | 44 | 52 | 18% | 0.008 |
| 55-59 | 48 | 57 | 19% | 0.02 |
| 60-64 | 46 | 61 | 33% | < 0.001 |
| 65-69 | 39 | 60 | 54% | < 0.001 |
Østerås' team also found fewer false-positive findings on DBT compared with digital mammography in all age and density groups, except for in women with extremely dense breasts.
| False-positive interpretations by modality, density, and age | ||||
| Patient characteristic | Digital mammography only (No. of cancers detected) | Digital mammography plus DBT (No. of cancers detected) | Percentage difference | p-value |
| All women | 2,466 | 2,081 | -15% | < 0.001 |
| Density | ||||
| Category 1 | 197 | 152 | -23% | 0.004 |
| Category 2 | 1,224 | 972 | -21% | < 0.001 |
| Category 3 | 815 | 721 | -12% | 0.004 |
| Category 4 | 229 | 234 | 2% | 0.82 |
| Age | ||||
| 50-54 | 901 | 800 | -11% | 0.002 |
| 55-59 | 619 | 542 | -12% | 0.009 |
| 60-64 | 521 | 388 | -26% | < 0.001 |
| 65-69 | 425 | 351 | -17% | 0.003 |
The study findings suggest that DBT is ready to be used as a standalone screening modality, wrote Drs. Michael Fuchsjäger and Gabriel Adelsmayr, both of the Medical University of Graz in Austria, in an accompanying editorial.
"We are currently amassing an ever-growing body of evidence on digital mammography plus DBT protocols, with the overall expected result that DBT adds value to digital mammography with greater cancer yield and reduction of recalls," they wrote. "Therefore, isn't it time to take this method to the next level and employ DBT as a stand-alone screening technique, combining it with automated three-dimensional ultrasound when necessary to create the supplemental screening 'dream team'? Having said that, it seems likely the next prospective trials are just around the corner."