Proton therapy is considered by some as the optimal radiation delivery modality -- with the finite range of protons enabling highly conformal dose targeting and reduced dose to normal tissue. Image guidance, using cone-beam CT (CBCT) for example, should increase the accuracy and improve outcomes further. But alongside, recent years have seen the emergence of online MR-guided radiotherapy, promising unparalleled soft-tissue image contrast and the ability to "see what you treat." In a theatrical debate at the recent European Society for Radiotherapy and Oncology (ESTRO) meeting, speakers considered whether proton-guided photons will be superior to photon-guided protons.
Bas Raaymakers, PhD, from University Medical Center Utrecht in the Netherlands, kicked off the debate by presenting the case for MRI-guided photon therapy. The first consideration, he said, is comparison of photons with protons. He described a fierce debate back in 2008 suggesting that in 10 years' time all radiotherapy will be delivered via protons. "That isn't going to happen," he pointed out.
 Bas Raaymakers and Tony Lomax held a lively debate at the ESTRO 36 meeting.
Bas Raaymakers and Tony Lomax held a lively debate at the ESTRO 36 meeting.One major obstacle is that protons are so much more expensive. A proton therapy installation starts at 30 million euros, while MR-guided radiotherapy systems cost around 6 million to 10 million euros. "People have asked whether protons are worth the investment," Raaymakers said. "It is a hard case to make."
Raaymakers explained that while there are currently 58 operational proton therapy facilities and another 52 on the way, the number of MR-guided radiotherapy systems is also increasing fast. "In a few years' time, we'll be at half the number of proton facilities," he predicted. "We're already way ahead of the number offering CBCT-guided protons. The ViewRay system has been treating patients since 2014, this is reality right now."
Another more pressing problem, Raaymakers suggested, is the high level of uncertainty associated with proton therapy, including uncertainties in range, dose calculation, beam modeling, and biology. "In reality, you can't exploit the Bragg peak because you don't know exactly where the range ends," he said, citing the common use of two opposing beams for prostate treatments, rather than daring to hit the tumor with the distal edge. "This is holding back proton progress."
He also noted the patients predicted to benefit most from proton therapy are those chosen to be treated. "This is very sensible, but also a sign that protons are not superior to the MR-linac at all, because you have to heavily select patients."
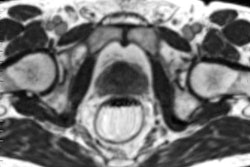
The second comparison to consider is MRI versus CBCT. "Either you can see virtually nothing prior to beam-on, or you can see everything during treatment. It's a no-brainer," Raaymakers said. "It's very hard to see what you need to using CBCT, while MRI can follow all deformations with time and really see what's going on during delivery."
Another benefit of MRI is the ability to reconstruct delivered dose distributions, and, if needed, create a completely new plan each day. This enables margin reduction, and, consequently, lower integral dose. "We have better alternatives than just the Bragg peak to reduce the dose," Raaymakers explained.
Proton promise
Arguing the case for CBCT-guided proton therapy, Tony Lomax, PhD, from the Paul Scherrer Institute in Villigen, Switzerland, took to the podium. "Proton-guided photons may reduce the margins, but photon-guided protons will reduce the volume of normal tissue receiving mid- to low-doses: the dose bath," he told the audience. "That bath may be low dose, but it is there and may be more significant than we think."
Lomax suggested that protons offer "a shower instead of a bath," and shared a host of examples demonstrating "the benefits of a good shower." First up, he cited a study comparing 558 proton therapy patients with 558 age-matched proton patients. The second cancer incidence at 10 years was 5.4% for patients treated with protons, compared with 8.6% for those receiving x-ray therapy. This factor-of-two difference mirrors the reduction in bath dose, he noted.
Another study examined pediatric medulloblastoma patients treated with protons or photons. Proton therapy significantly reduced adverse effects, resulting in a 2.8-times reduction in hypothyroidism (23% versus 65% for photon irradiation), a 6.3-times reduction in sex hormone deficiency (3% versus 19%), and a 1.4-times reduction in the need for endocrine replacement therapy (55% versus 78%).
Elsewhere, a study of children with brain tumors treated with protons or photons showed that proton therapy can improve quality-of-life (QoL) after treatment. "The health-related QoL was close to that of normal controls for proton patients, while for photon patients it was reduced," Lomax explained.
To illustrate the adverse consequences of the dose bath, he described some animal studies. For example, irradiating rats' parotid glands showed that a 1 Gy added dose bath led to 30% reduced parotid flow. Meanwhile, adding a 4 Gy dose bath when irradiating a rat's spinal cord reduced spinal cord tolerance by 25%.
Lomax also described a study in which the distal edge was employed to spare nearby organs-at-risk. High-dose scanned protons were used to treat 31 paraspinal/retroperitoneal tumors, a malignancy where dose was historically limited by small bowel dose constraints. Despite target doses of more than 70 Gy (RBE), no acute toxicities were observed, with just one patient suffering a grade 1 toxicity. "We're basically putting no dose into the rest of the bowel so there's virtually no toxicity," Lomax said. "This is the power of the shower."
Likewise, in a study of 222 patients with skull-base chordomas treated with pencil-beam scanned protons, not one brainstem toxicity was seen. "I don't believe any of these indications would benefit from treatment with the MR-linac," Lomax noted.
The delegates decide
At this point, the session chairs polled the audience using what chair Joseph Deasy described as an "intensity-modulated voting system." The audience voted convincingly for photon-guided protons, creating a noise level of 82 dB (as measured by co-chair Jan-Jakob Sonke) compared with 75 dB for proton-guided photons.
But the story doesn't end there. The speakers returned to the podium to present their rebuttals. Raaymakers emphasized that, right now, the main aim is to deliver conformal dose to target. While a low overall dose is obviously advantageous, if a target lies next to a sensitive organ, then using MRI to reduce margins can give a smaller high-dose area and less dose-limiting toxicities. "First we have to solve the geometric challenge, then bring in the biology," he said, pointing out that if you can visualize the delivered dose, this can be correlated with toxicities to help understand the biology.
"Clearly there are cases where proton therapy can do a better job; brain and pediatric patients need best the treatment, of course," Raaymakers concurred. "But we need to treat all cases, we need a general purpose better radiotherapy. MR-guided radiotherapy will be the workhorse."


Estimated numbers of new cancer cases (incidence) and deaths (mortality) in (a) men and (b) women in more developed and less developed regions of the world in 2012. Reprinted from J Ferlay, International Journal of Cancer, 136 E359 © 2014 UICC.
"I agree that we need to see the target," Lomax replied. "But do we need to do MR online?" He pointed out it is possible to perform MRI offline and create patient-specific motion models. Combining such models with images of a surrogate during treatment enables target motion prediction to within about 2 mm.
"I personally look forward to seeing future clinical results from both proton-guided photons and photon-guided protons, as well as proton-guided protons and even phonon-guided protons and photons," Lomax concluded. "Let's come back in 10 years' time and see where we are."
A final intensity-modulated vote revealed a change of heart from the audience, with fans of photon-guided protons registering 81 dB and those choosing proton-guided photons reaching 82 dB. Perhaps the future does indeed lie in MR-guided radiotherapy -- or maybe its proponents can just cheer louder.
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community website covering fundamental research and emerging technologies in medical imaging and radiation therapy.