MR spectroscopy can be a useful adjunct for differential diagnosis of intracranial hydatid disease, a rare zoonosis caused by the Ehinococcus tapeworm, according to a case report published online on 12 September in BMJ Case Reports.
Dr. Bedros Taslakian of New York University Langone Medical Center in New York City and Dr. Houssein Darwish of American University of Beirut Medical Center reported on the imaging findings of a 12-year-old boy who presented with headaches and vomiting for a few months. The boy was diagnosed with an intracranial hydatid cyst, which was totally excised with no postoperative complications.
Diagnosing a hydatid cyst can be challenging, especially when serological tests are negative. As a result, it's important to understand the imaging presentation of this rare disease, which is endemic in areas of the world such as the Middle East, Australia, New Zealand, South America, and central and south Europe, according to the authors.
"The differential diagnosis of intracranial cystic lesions is wide, including cystic and necrotic malignancies, as well as a wide range of benign lesions such as abscesses," they wrote. "Differentiating these lesions is essential in the management and can be at times difficult."
CT and MRI are currently considered the most reliable means of preoperative means of diagnosing hydatid cysts.
"Although CT is superior in detecting calcification of the cyst wall, when present, MRI is better in detecting multiplicity and defining the anatomic relationship of the lesion with the adjacent structures and helps in surgical planning," the authors wrote. "The MR spectroscopy findings of the present case were specific to what may be present in cases of hydatid disease of the brain."
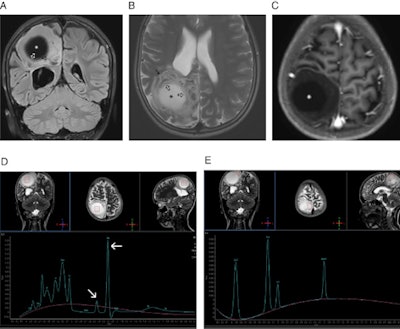
 A: Coronal fluid attenuation inversion-recovery (FLAIR) MRI of the brain showing a large, well-defined, unilocular, cerebrospinal fluid-like cyst (*) located in the right parietal lobe. The cyst is causing minimal mass effect on the occipital horn of the right lateral ventricle (arrow) with mild surrounding vasogenic edema. Collapsed membranes are seen in the medial and inferior aspect of the cyst (open arrows). B: Axial T2-weighted MRI of the brain showing the right parietal hyperintense hydatid cyst (*). The cyst has a thin hypointense rim (arrow) with mild surrounding vasogenic edema along its anterior aspect. Collapsed membranes are seen in its medial aspect with a ball-of-wool pattern (open arrows). C: Axial T1-weighted MRI of the brain after gadolinium administration showing the right parietal hypointense hydatid cyst (*) with the nonenhancing collapsed membranes seen in its medial aspect. D: Single-voxel MR spectroscopy from the central cystic portion of the lesion showing increased choline, a small peak at 2.40-2.50 ppm representing pyruvate and succinate (oblique arrow), and a large abnormal peak at 2.2 ppm representing glutamate/amino acids (horizontal arrow). Pyruvate and succinate are well-known metabolic end products arising from microorganisms. E: Single-voxel MR spectroscopy from the peripheral solid portion of the cystic lesion showing increased choline/N-acetyl aspartate ratio. All images courtesy of BMJ Case Reports.
A: Coronal fluid attenuation inversion-recovery (FLAIR) MRI of the brain showing a large, well-defined, unilocular, cerebrospinal fluid-like cyst (*) located in the right parietal lobe. The cyst is causing minimal mass effect on the occipital horn of the right lateral ventricle (arrow) with mild surrounding vasogenic edema. Collapsed membranes are seen in the medial and inferior aspect of the cyst (open arrows). B: Axial T2-weighted MRI of the brain showing the right parietal hyperintense hydatid cyst (*). The cyst has a thin hypointense rim (arrow) with mild surrounding vasogenic edema along its anterior aspect. Collapsed membranes are seen in its medial aspect with a ball-of-wool pattern (open arrows). C: Axial T1-weighted MRI of the brain after gadolinium administration showing the right parietal hypointense hydatid cyst (*) with the nonenhancing collapsed membranes seen in its medial aspect. D: Single-voxel MR spectroscopy from the central cystic portion of the lesion showing increased choline, a small peak at 2.40-2.50 ppm representing pyruvate and succinate (oblique arrow), and a large abnormal peak at 2.2 ppm representing glutamate/amino acids (horizontal arrow). Pyruvate and succinate are well-known metabolic end products arising from microorganisms. E: Single-voxel MR spectroscopy from the peripheral solid portion of the cystic lesion showing increased choline/N-acetyl aspartate ratio. All images courtesy of BMJ Case Reports.In this case, MR spectroscopy of the central cystic part of the lesion demonstrated elevated choline, as well as pyruvate and succinate picks, while also showed an increased choline/N-acetyl-aspartate (NAA) ratio and a large peak of lipids, according to the authors.
"As proton MR spectroscopy provides a noninvasive method for examining a wide variety of metabolites in the human brain, it can be used as an adjunctive modality to identify the nature of intracranial lesions including hydatid cysts," they wrote.