Emerging 3D printing techniques offer great potential to improve interventional radiology training by the use of custom-built rubberlike vessel phantoms that can simulate even the complex anatomy of patients, according to award-winning research from Germany.
A team from Munich, headed by Dr. Marcus Treitl from the Institute for Clinical Radiology at the Ludwig-Maximilians University, aimed to describe and compare the various methods for composing and building vessel models for real-life simulation. They received a Certificate of Merit award for their e-poster presentation at the RSNA 2014 meeting in Chicago.
Training of endovascular skills must improve, according to the authors. Not only are interventional radiology and endovascular techniques rapidly growing fields, but every year there are new things to learn, new procedures (aneurysms, prostatic, etc.), and new materials (liquids, coils, stents, stent-grafts, plugs).
Keeping up with developments in the field becomes more and more difficult, and timely training of staff and young academics can be impossible, they added. Sometimes, however, there are only small patient counts for special procedures or materials.
Among the possible solutions to this problem are:
Training in other centers, or working abroad as visiting observers. Staff and young academics are sent to centers dedicated to a special procedure for state-of-the art training with an opinion leader, but this is time-consuming and it results in a lack of personnel in the trainee's own department during the observational period. Also, training can only be given in a limited number of procedures, and several different observational visits are necessary to train the entire staff.
Training with electronic simulators. Sophisticated, close-to-reality, "black hole" simulators can be used for training in different endovascular procedures, but they are too expensive for most departments and not all kinds of procedures can be taught. It also takes a while until new procedures are implemented, there is no possibility to give training in a certain material/catheter, and information about behavior of materials gets lost and only the endovascular part can be simulated.
Training with artificial vessel phantoms in the cath lab. Vessel phantoms made from a rubberlike material and connected to a flow-simulator can be used to train endovascular procedures under real conditions with real materials and under fluoroscopy. Training in different materials and different vessel anatomies can be given. They are less expensive than electronic simulators, and real anatomy of an upcoming patient can be simulated. Training is provided in-house, and no additional personnel are required. However, it is not really implemented yet, only a few companies offer production of custom-made vessel phantoms, and a variety of possible materials exists.
Industrially produced silicone vessel phantoms now exist, and several companies offer ready-made silicone aortic models, noted Treitl et al. Perfect shapes are available easily for well-established systems, but they are very expensive and they are not really a viable alternative because models will get destroyed during training and costs will escalate.
As for custom-made semi-industrial silicone phantoms, emerging companies can offer 3D-printing with siliconelike rubber material that requires a customer-derived model file for printing, but they are still expensive and time-consuming, they explained.
Completely self-made silicone-vessel phantoms are another option. In-house 3D printing with low-to-medium cost 3D printers is possible for various anatomies and it requires little investment in 3D printing or silicone lab equipment, but it is time-consuming in the case of completely handmade models.
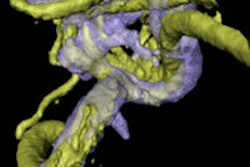
Self-made vessel phantoms offer the possibility for 3D CT angiography scans of the vessel anatomy to be obtained for 3D printing using software to make 3D segmentation of the desired vessel area. A lab for silicone works in the case of completely hand-made silicone models, and a 3D printer can be used for in-house production, the authors continued.
For rendering and segmentation of the CT dataset, various software packages are available, and they run the gamut from low to high cost. The requirements for this type of software are an option for 3D segmentation of the vasculature, an ability to make .stl (stereo-lithography) files for 3D printing out of the segmented 3D dataset, the Mimics Innovation suite, and a complete package, including 3D CAD design software to additionally adjust the model file. Other packages are available from various vendors.
For making handmade silicone models, a mold is necessary to reproduce the model as often as desired, they noted. For mold production, a primary wax model based on the real anatomy is necessary. The first wax model is used to build a silicone mold. For reproduction, the mold will be filled with a low-melting casting wax, which afterwards will be used to make the final silicone vessel.
To make the final silicone model, the low-melting wax model from the previous step is covered with silicone until the desired wall thickness has been reached. Liquid silicone is used to cover the wax model. The final silicone-vessel phantom is obtained after melting out the wax core in hot water.
According to Treitl et al, 3D printing is one of the fastest-growing new technologies of the last five years, and several very different printing techniques are available, including stereo lithography and film transfer imaging (FTI). Often used in medium-cost 3D printers, it is very precise but also error-prone. Fused deposition modeling (FDM) is mostly seen in low-cost desktop 3D printers, and a broad variety of low-cost materials can be experimented with. Medium-cost 3D printers like the ProJet 1500 machine uses plastic-like material, called VisiJet.
A third-party 3D printing service is highly flexible but not very stress-resistant, they stated. The HeartPrint flex is still expensive (about $1,000 U.S. to $1,500 U.S. or 880 euros to 1,300 euros). Hand-made silicone models are cheaper, but are very time-consuming and therefore expensive (around $900 U.S. or 800 euros for the first mold, and then $200 U.S. or 175 euros). Self-3D-printed models can be cheaper, but require higher first-time investments (about $100 U.S. per model; $10,000 U.S. or 8,800 euros for a medium-cost printer, and $2,000 U.S. or 1,760 euros for a low-cost printer).
"Rapid developments in catheters, materials, and techniques hinder comprehensive training of staff and young academics. Observational visits and electronic simulators are not a suitable long-term solution," the authors concluded. "Rubberlike vessel phantoms offer a possibility to train and teach materials and techniques in a real-life setting."