What should you do when you find a calcified lesion on an abdominal x-ray? Should you do nothing because the diagnosis is complete, or should you do a CT or another supplementary examination? To answer tricky questions like these, it's vital to learn how and when to diagnose calcified lesions on plain film and to recognize those cases where another examination is required, according to radiologists from Spain.
"Once upon a time, before CT development, fearless radiologists made their diagnosis using primitive tools such as radiography, clinical inspection, deduction, and a little bit of imagination," noted Dr. Alvaro Paniagua Bravo, and colleagues from the Unidad Central de Radiodiagnóstico, Hospital Infanta Sofía in Madrid, in research presented at RSNA 2014 in Chicago. "This presentation is dedicated to those earnest pioneers of radiology."
Plain film is used for abdominal occlusion evaluation and urolithiasis detection, but often it is not a great tool for evaluation of unspecific abdominal pain. Many calcified lesions are nonpathological findings that do not need any additional study, especially when the patient is asymptomatic, but when diagnosis is not clear on plain film, ultrasound or CT should be the next step, they advised.
A gallstone (also called cholelithiasis) is a crystalline concretion formed within the gallbladder by accretion of bile components. Because gallstones are radiopaque only in 15% to 20% of cases, ultrasound is the method of choice for detection, but sometimes they can be seen on plain film with a characteristic shape and location.
Porcelain gallbladder is an uncommon manifestation of chronic cholecystitis, characterized by intramural calcification of the gallbladder wall. Patients with a porcelain gallbladder are often asymptomatic, but are at increased risk for the development of gallbladder carcinoma. There are different classifications based on gallstones composition and appearance, although a reliable relationship between radiological appearance and stone composition has not been found, explained the authors.
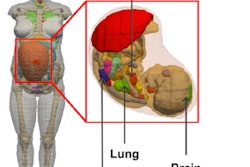
Hydatid disease often affects the liver, and abdominal plain films may visualize fluid density cysts, with frequent peripheral focal areas of calcification, septation, and daughter cysts.
"Tortuosity and splenic wall calcification is a common finding in abdominal plain x-ray," they stated in an e-poster. "Usually morphology is quite obvious and does not need further examinations; however, sometimes it can be confused with renal lithiasis or calcified adenopathy."
The incidence of splenic artery aneurysms is about 1% in the general population, and most patients are asymptomatic. Partial or complete calcification in the walls of the aneurysm can be seen in plain film, according to Paniagua Bravo and colleagues. Treatment is indicated for aneurysms that cause symptoms, are more than 30 mm in diameter, and in women who are pregnant or of child-bearing age. In such cases, a CT scan should be carried out for better evaluation.
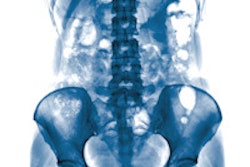
Renal stones are composed of a combination of crystals and proteins, and the most common symptom in patients with urolithiasis is acute flank pain. As the sole imaging modality for the evaluation of nephrolithiasis, conventional abdominal radiography is limited by several factors, including bowel gas, extrarenal calcification, and large patient habitus, but it is useful for initial diagnosis, planning fluoroscopically guided lithotripsy, and monitoring the status of stone fragments.
| Right/left lumbar region: Nephrolithiasis | |||
| Composition | Frequency | Radiographic appearance | CT appearance |
| Calicum oxalate | 40% to 60% | Radiopaque | Opacified (1,700-2,800 HU) |
| Hydroxyapatite | 20% to 60% | Radiopaque | Opacified (1,200-1,600 HU) |
| Uric acid | 5% to 10% | Radiolucent | Opacified (200-450 HU) |
| Struvite | 5% to 15% | Radiopaque | Opacified (600-900 HU) |
| Brushite | 2% to 4% | Radiopaque | Opacified (1,700-2,800 HU) |
| Cystine | 1% to 2% | Mildly opaque | Opacified (600-1,100 HU) |
"Abdominal plain film can show calcium oxalate lithiasis in both kidneys, and this can be confirmed with renal ultrasound and pathological analysis after expulsion," they reported.
Other points to bear in mind are the following:
Coral calculi, also called staghorn calculi, are composed of struvite (magnesium ammonium phosphate) and are usually seen in the setting of infection with urease-producing bacteria. The vast majority of coral calculi is radiopaque, and appear as branching calcific densities that conform to the renal pelvis and calyces.
Calcified aortic wall is a typical finding on abdominal plain film, especially in elderly patients. Aortic aneurysm can be detected when the wall is calcified. CT can confirm the diagnosis and allow aneurysm measurement.
An appendicolith, which is a calcified deposit within the appendix, is present in many children with acute appendicitis, but also may be an incidental finding on an abdominal radiograph or CT scan. Only when associated with abdominal pain is there a high probability of acute appendicitis.
Gallstone ileus, caused by impaction of a gallstone in the ileum after being passed through a biliary-enteric fistula, is rarely seen on x-ray film, but CT can confirm the ileal location. Gas in the gallbladder, when present, helps the diagnosis.
Uterine myoma, or uterine fibroid, is the most common benign gynecologic tumors. Popcorn calcification within the pelvis may suggest the diagnosis, and it is a common finding on abdominal plain film.
A phlebolith is a small, local, usually rounded, calcification within a vein. These are very common in the veins of the lower part of the pelvis, and they are generally of no clinical importance. When located in the pelvis, they can be difficult to differentiate from kidney stones in the ureter on x-ray. Phleboliths appear as focal calcifications, often with radiolucent centers, which distinguish them from ureteric calculi. This appearance is attributed to calcification peripherally within the vessel. The amount of phleboliths increases with age and they also appear more often on the left than on the right side of the pelvic region.
"Uterine myoma and phleboliths are the most common findings in the hypogastric region on abdominal plain film. Usually they are harmless and do not need subsequent studies," the authors noted.
The Madrid group's other recommendations are as follows:
Gluteal injection site granulomas are a very common finding on CT and plain film. They occur as a result of subcutaneous injection of drugs, which cause localized fat necrosis, scar formation, and dystrophic calcification. Once a radiologist is familiar with them, they rarely pose any diagnostic confusion.
Ovarian teratomas are a common germ cell neoplasm that contain mature tissues of ectodermal (skin, brain), mesodermal (muscle, fat), and endodermal (mucinous or ciliated epithelium) origin. The presence of calcium in the tumor allows its detection on x-ray in the hypogastric or right/left iliac region, but a gynecologic exam with ultrasound and sometimes CT is recommended.
Pregnancy may be an incidental finding. A very unusual entity to consider is lithopedion, which is a rare phenomenon occurring most commonly when a fetus dies during an abdominal pregnancy and is too large to be reabsorbed by the body and calcifies.
Be aware of external devices. For instance, the top of a urinary catheter may simulate a pelvic calcification.