Abdominal CT with compression to the right lower quadrant (RLQ) has a high diagnostic accuracy in cases of acute appendicitis, and can be considered as a CT counterpart of graded compression ultrasound, Turkish researchers reported at the recent RSNA 2014 meeting.
The presence of persistent RLQ pain and a noncompressible appendix with an outer appendiceal diameter greater than 6 mm can lead to a diagnosis of acute appendicitis using the ultrasound-graded compression technique. However, the main limitations for ultrasound evaluation are obesity and intestinal gas superposition, especially in cases of retrocecal appendicitis, and CT is preferred in such patients, according to Dr. Erhan Akpinar and colleagues from the department of radiology at Hacettepe University in Ankara.
In abdominal CT examinations, some patients have a normal appendix with an outer diameter greater than 6 mm. The Turkish group thinks this fact is related to the absence of compression in routine abdominal CT studies.
"Does compression to the RLQ affect the appendix outer diameter or the appendiceal luminal content?" asked Akpinar et al, who sought to determine the diagnostic accuracy of abdominal CT with compression to RLQ in adults for the diagnosis of acute appendicitis.


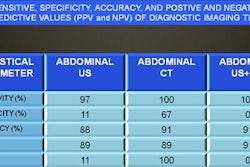
CT and ultrasound compared in cases of acute appendicitis and perforated appendix.
In their study, presented as an e-poster, 168 patients (114 women and 54 men with a mean age of 35.7 and age range of 18-78) underwent contrast-enhanced CT for suspected appendicitis. Compression CT was used in 71 patients between July 2012 and September 2013. Standard abdominal CT was used in 97 patients between April 2011 and June 2012. All the patients in the former group had an abdominal ultrasound examination before CT to exclude conditions like abdominal aortic aneurysm and urinary obstruction. Institutional review board approval was obtained, and patients in the compression group were asked to give their written informed consent.
Oral and intravenous iodinated contrast media were used in compression CT exams. Compression of the RLQ was achieved with a 1,000 cc saline bag and a 26 x 75 cm elastic belt with Velcro strips. From the top of the diaphragm to the base of the symphysis pubis, 5-mm-thick transverse sections were obtained in the venous phase, using either a 2- or 16-detector row CT scanner (Emotion Duo and Somatom Sensation 16, Siemens Healthcare). From the raw data of each acquisition obtained with the 16-detector row CT system (55 of 71 patients), transverse sections were reconstructed at 2-mm slice thickness and 1-mm intervals to perform multiplanar reconstructions.
In the standard abdominal CT exams, oral and intravenous iodinated contrast material was used, and images were obtained in the venous phase without any compression on a 2- or 16-detector row CT (85 and 12 patients, respectively). All images were created only with 5-mm slice thickness, and the other technical parameters and anatomical coverage were constant.
For the image interpretation, the outer diameter of the appendix, wall thickening and enhancement, periappendiceal inflammatory changes, and appendiceal luminal content were assessed for each patient. Two radiologists reviewed CT images, and the final diagnosis was based on pathologic verification and/or definitive diagnosis at discharge.
In the compression CT group (62 cases), acute appendicitis was diagnosed in 23 patients, and the appendix was normal in 39 patients. In the standard abdominal CT group (91 cases), acute appendicitis was found in 35 patients, and the appendix was normal in 56 patients. A total of 15 patients (nine compression CT and six standard abdominal CT) were excluded from the study due to a lack of pathologic proof.
 Study results for the appendiceal lumen. Filling of contrast material to the appendiceal lumen was statistically higher in compression group when compared with standard abdomen CT group (p < 0.01).
Study results for the appendiceal lumen. Filling of contrast material to the appendiceal lumen was statistically higher in compression group when compared with standard abdomen CT group (p < 0.01).The most significant and powerful finding in the ultrasonographic graded compression technique was a tubular structure that is not compressible, the authors noted. An ovoid shape of the appendix in the ultrasound exam helps to reliably rule out acute appendicitis, and in routine abdominal CT exams, this feature cannot be evaluated, they added.
Normal appendix diameter was significantly smaller in the compression CT group when compared with the standard CT group, Akpinar and colleagues concluded. Filling of contrast material to the appendiceal lumen was statistically higher in the compression CT group when compared with the standard CT group.