The U.K. Royal College of Radiologists (RCR) has published updated recommendations for the safe use of coronary CT angiography (CCTA) in the investigation of patients with chest pain. The 26-page document can be downloaded for free from the RCR's website and includes practical information about image quality, radiation dose, and patient safety.
Close links with referring clinical teams are essential, and a clear understanding of how the scan is performed and the information it is capable of providing will mean that appropriate patients are referred for a CCTA scan. A statement on the referral letter or request card about no known contraindications to betablockers, glyceryl trinitrate, or intravenous contrast medium is very helpful, but does not obviate the need for safety checks, the authors explained.
"It is also important that the referring clinical team is aware that this test involves ionizing radiation. The referrer and the imaging team must follow the ionizing radiation medical exposure regulations (IRMER) procedures for carrying out medical exposures with ionizing radiation," they stated. "A medical member of the imaging team will act as the IRMER practitioner and will be responsible for confirming that the investigation and the associated radiation dose can be justified."
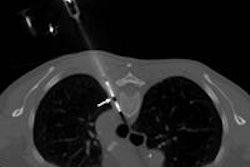
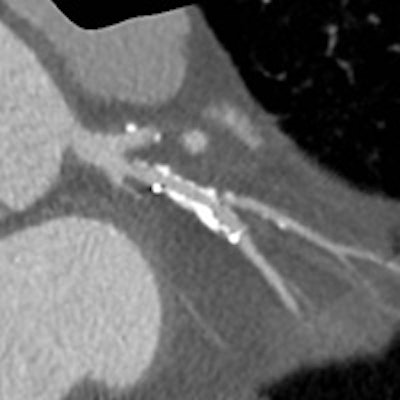
 Comparison images demonstrating how high-definition CT angiograpy improved reporting accuracy. The case is of a 49-year-old man with previous stent to the circumflex artery with recurrent pain. New scanner technology allows the use of CCTA in patients with known existing heart disease and gives the interventional cardiologist the required information to plan the subsequent intervention. Top left image shows a stent in the circumflex artery but no stenosis. Bottom left shows an occluded right coronary. Top middle also is of the circumflex but demonstrates how the use of the Discovery CT750 HD scanner (GE Healthcare) allows clear visualization of the short stenosis, despite the stent and high level of calcium in the arteries. Top right is a conventional left coronary angiogram confirming the CT findings. Bottom right is the right coronary angiogram confirming findings. All images courtesy of Dr. Carl Roobottom, Plymouth University Hospital, U.K.
Comparison images demonstrating how high-definition CT angiograpy improved reporting accuracy. The case is of a 49-year-old man with previous stent to the circumflex artery with recurrent pain. New scanner technology allows the use of CCTA in patients with known existing heart disease and gives the interventional cardiologist the required information to plan the subsequent intervention. Top left image shows a stent in the circumflex artery but no stenosis. Bottom left shows an occluded right coronary. Top middle also is of the circumflex but demonstrates how the use of the Discovery CT750 HD scanner (GE Healthcare) allows clear visualization of the short stenosis, despite the stent and high level of calcium in the arteries. Top right is a conventional left coronary angiogram confirming the CT findings. Bottom right is the right coronary angiogram confirming findings. All images courtesy of Dr. Carl Roobottom, Plymouth University Hospital, U.K.Produced in association with the Royal College of Physicians and the British Society of Cardiovascular Imaging, the new edition (Ref No: BFCR[14]16) is divided into sections of recommended best practice before the start of the scan, during the scan, and once the scan has been completed. The document brings together the latest guidance on departmental standards of practice required to deliver safe CCTA to adult patients.
 Dr. Stephen Harden was chair of the working party that developed the new document.
Dr. Stephen Harden was chair of the working party that developed the new document.The patient should wait in the department for 15 minutes before leaving, or 30 minutes if there is an increased risk of contrast reaction. Getting formal feedback is also important, and may take the form of a patient satisfaction survey or a patient experience questionnaire.
The emphasis should be on achieving a good procedural outcome, with diagnostic quality images obtained in an environment in which the safety of the patient is paramount, and radiologists must be aware of the potential complications and interactions of heart rate controlling drugs and intravenous contrast media, noted the authors. All staff should have frequent and up-to-date training in basic life support, and at least one member of the team should be trained in immediate life support. Resuscitation facilities should be immediately available.
The other key recommendations are as follows:
All patients should receive a letter/information leaflet giving an outline of the procedure, the preparation required, and local site details. They should have a risk assessment undertaken by a member of staff.
Provided it is safe and practical to do so, heart rate controlling drugs should be administered so the patient's heart rate is less than 65 beats per minute during the scan.
The scanner should be specifically set up for CCTA and be of 64 slices or greater, with cardiac software and electrocardiogram gating.
Prospective ECG gating should be the first-line default technique, used whenever possible and practical. Retrospective ECG gating should only be used in specifically selected cases.
The radiation dose administered should be as low as possible, commensurate with diagnostic image quality. Radiation doses and imaging quality should be routinely and regularly audited and benchmarked against other national centers.
The iodinated contrast medium delivery protocol should be adjusted for each patient group and according to the scanner being used.
The patient should be reviewed by an appropriately qualified member of staff prior to discharge from the scanning department.
"Appropriate training of all healthcare professionals involved in delivering coronary CT angiography to adult patients with known or suspected coronary artery disease is essential, together with the most appropriate and up-to-date CT scanners with the ability to modulate dose," noted Dr. Pete Cavanagh, the RCR's vice president for clinical radiology, in the foreword.
For more details on the guidelines click here.
Editor's note: Following the RCR's Annual General Meeting in September, Dr. Pete Cavanagh is no longer vice president for clinical radiology, although he would have been when the document was written. Dr. Richard Fitzgerald is the new vice president for clinical radiology. As many of you know, Fitzgerald was an active member of AuntMinnieEurope.com's editorial advisory board until he stepped down last year.