Radiation dose may be reduced by 32% in digital chest tomosynthesis without significantly altering the technique's ability to detect pulmonary nodules, according to a study out of Sweden. The researchers were able to decrease the radiation dose of tomosynthesis to the level of a lateral chest radiograph.
Chest tomosynthesis involves reconstructing low-dose projections acquired over a limited angular range into a 3D image of the chest. The technique offers improvements over conventional radiography in visualizing pathology that might be obstructed by anatomy (European Radiology, 4 May 2014).
The radiation dose of tomosynthesis is much lower than that of CT, but it is still higher than the dose from conventional x-ray. However, recent phantom studies have shown that chest tomosynthesis dose could be reduced to 0.14 mSv to 0.06 mSv without decreasing nodule detection for nodules larger than 4 mm. An effective tomosynthesis dose range of 0.1 mSv to 0.2 mSv has been reported, which is slightly higher than the 0.04 mSv to 0.1 mSv typically reported for chest radiography.
"The performance of tomosynthesis operated at a reduced dose level ... has, however, not been investigated in real patients," wrote Sara Asplund, a PhD student in the department of radiation physics at Sahlgrenska Academy at the University of Gothenburg, and colleagues. "Thus, the purpose of the present study was to investigate the effect of radiation dose level on the detection of pulmonary nodules in chest tomosynthesis using patient images with added artificial noise."
The researchers included 86 patients who were examined with tomosynthesis (VolumeRad, GE Healthcare) and CT (LightSpeed Pro 16 and LightSpeed VCT, GE). Artificial noise was added to simulate that the tomosynthesis images were acquired at dose levels corresponding to 12%, 32%, and 70% of the default setting effective dose (0.12 mSv). Three observers read the tomosynthesis cases for the presence of nodules in a free-response receiver operator characteristics (FROC) analysis. CT served as a reference.
Differences between dose levels were calculated using the jackknife alternative FROC (JAFROC) figure of merit (FOM). The group found that JAFROC FOM was 0.45, 0.54, 0.55, and 0.54 for the 12%, 32%, 70%, and 100% dose levels, respectively. The differences in FOM between the 12% dose level and the 32%, 70%, and 100% dose levels were 0.087, 0.099, and 0.093, respectively. No significant differences were found between higher dose levels, the authors wrote.
"As chest tomosynthesis recently has been introduced to healthcare, the effects of radiation dose reduction for this modality have not yet been fully evaluated," they wrote. "In the present study, the effect of the radiation dose level on the detectability of pulmonary nodules was investigated. For this task, the results of the JAFROC analysis showed no statistically significant differences between the three highest dose levels."
Asplund and colleagues admit that a large proportion of the nodules in the present study were not visible with tomosynthesis, especially nodules 4 mm or smaller, of which only 52% (96 out of 186) were visible. However, the clinical relevance is limited for this size of nodules compared with the intermediate and large nodules -- of which 85% (60 out of 71) were visible.
"This indicates that tomosynthesis may be used for follow-up of known nodules, as has been suggested by previous studies," they wrote.
For nodules 4 mm or smaller, no significant differences in JAFROC FOM were found between any of the dose levels. This may seem surprising, considering a dose reduction presumably would influence the detection of small nodules more (probably resulting in larger differences in FOM between dose levels) than larger nodules, the researchers noted.
"Also, as the number of small nodules was higher than the number of larger nodules (for which significant statistical differences were found), a higher statistical power could have been expected for the analysis of the small nodules," they added. "However, the lesion localization fraction for small nodules was generally low regardless of dose level, even though the nodules were visible on the tomosynthesis images."
Compared with the 100% dose level, data presented in an evaluation of the simulated dose reduction method can be interpreted as a reduction in total detective quantum efficiency (DQE) by 5%, 20%, and 60% at the 70%, 32%, and 12% levels.
"Thus, the increase in image noise at the lower dose levels is higher than anticipated from the reduction in dose per se; at the lowest dose level the image noise corresponds to a reduction in dose by 95%, had the DQE been unaffected by the dose reduction. Also, at lower dose levels the DQE drops more quickly with spatial frequency, meaning that the low-dose images contain more fine-structured noise, possibly affecting the nodule detection."
Clinical practice
In clinical practice, the possible dose reduction is constrained by the inability of the x-ray tube to provide an output lower than 0.25 mAs per projection image; however, the tube voltage can be lowered, enabling higher tube loads at a given effective dose.
The researchers caution that as the ratio between the detector dose and the effective dose is decreased for lower tube voltages, this dose reduction method may lead to additional noise due to the decrease in DQE at lower detector doses, despite the fact that DQE at constant detector doses in general may be higher at lower tube voltages.
Another possibility is to combine a reduced tube voltage with additional filtration, and this may also have the additional advantage of further reducing the risk of reaching the minimum tube load limit when trying to implement a dose reduction clinically, the researchers wrote.
"In the present study, the images were dose-reduced to the same level as a lateral projection in a standard chest radiography examination (32% of the default tomosynthesis dose) without a significant decrease in detectability," they added. "However, the detectability of nodules in tomosynthesis performed at this dose level compared to the lateral projection has not yet been investigated."
Even so, considering the superiority of tomosynthesis over radiography shown in several studies, replacing the lateral view of conventional radiography with tomosynthesis in selected cases may be appropriate for specific tasks, they concluded.
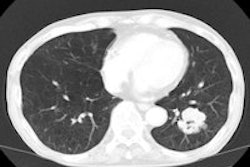
Editor's note: The image on the home page is of a 65-year-old man with a peripheral pulmonary ground-glass pulmonary nodule. Digital tomosynthesis planes show a ground-glass pulmonary nodule (arrow) with evidence of intralesional air bronchogram. Image courtesy of Dr. Emilio Quaia.