In the wake of the Poly Implant Prothese (PIP) breast implant scandal, MRI has proved to be of great value in diagnosing postsurgical complications, and it is now becoming the modality of choice for investigating the malfunctioning penile prosthesis, according to award-winning research from the U.K.
MRI is particularly useful for evaluating painful penile implants, given its high sensitivity for determining abnormalities and its superiority over physical examinations when complications exist, noted Dr. Fiona Pathiraja, a specialist registrar in radiology, and colleagues from University College London (UCL).
"Complications of penile implants can have serious ramifications on the physical and psychological health and well-being of patients," they stated in an ECR 2014 e-poster presentation that received a cum laude award. "Complications of penile implants usually relate to one of three categories: implantation, infection, or mechanical failure of prosthesis."
 A diagram depicting the three main categories of complications that occur in penile implants. Source: Dr. Fiona Pathiraja, University College London, presented at ECR 2014.
A diagram depicting the three main categories of complications that occur in penile implants. Source: Dr. Fiona Pathiraja, University College London, presented at ECR 2014.There are two main types of penile implants used for patients with erectile dysfunction: complex inflatable implants and the more simple semirigid malleable implants. The former include two penile cylinders, a pump within the scrotum, and a reservoir in the prevesical space; and the device allows both flaccidity and erection, the authors explained. Malleable implants, on the other hand, comprise noninflatable malleable rods, and they are simpler to implant but are semirigid at all times and do not allow complete flaccidity.
"Penile implants have high patient satisfaction rates. However, they do present complications," wrote Pathiraja et al.
At UCL, standard sequences for penile MRI involve high resolution (matrix size 200 or greater), small field-of-view, thin-slice (ideally 3 mm) T2-weighted spin echo sequences in three orthogonal planes. During the examination, the penis is in the anatomical position, resting on the anterior abdominal wall in the midline, though to minimize breathing artifacts, it may be placed dependently.
MRI can outline the position of both malleable and inflatable implants, the authors noted. Inflatable implants are seen best on T2 and short-tau inversion recovery (STIR) sequences, and they recommend scanning with the device inflated when possible. Ultrasound is adequate in many cases to check for fluid in the device, but several abnormalities are visualized best on MRI. Imaging in the absence of full implant inflation can give the false impression of implant buckling.
For malleable implants, additional sequences are used where necessary, depending upon the clinical indication, they continued. These include T1-weighted images, which may be useful for the detection of hemorrhage and thrombosis within the corpora or draining veins. Small field-of-view STIR sequences may show inflammation, and sometimes the deep veins of the pelvis well. The role of contrast enhancement in the detection of infection has not been examined.
The following complications may occur:
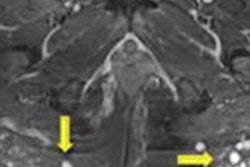
Buckling, due to overly long prosthesis, is more common than crossover and can cause pain during inflation. In a study of patients who experienced pain more than two months after implantation, an abnormality was identified at MRI in all 14 patients, whilst physical examination determined an abnormality in only five cases, according to the authors.
Crossover of cavernosal components is relatively rare, but seen well on MRI.
Infection occurs in around 2% to 4% of inflatable implants, though subclinical infection is more common. It is often associated with periprosthetic fluid and stranding (seen in particular on STIR sequences), though these findings should be interpreted with caution: Some fluid does not necessarily imply infection, and stranding may be seen for several months after insertion. Infections that are shown clearly on MRI are usually clinically apparent as well. Infection may affect the cylinders, reservoir, or the pump, they added.
Mechanical failure rates have decreased considerably in 30 years and are less than 10% at five years with most devices.
Herniation or displacement of parts of the prosthesis or its supporting parts.
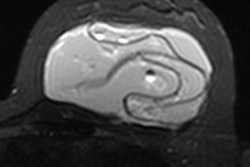
Aneurysmal dilatation of the cavernosal components is visualized well, and may lead to bulge and underinflation.
Leakage of the inflatable cylinders occurs rarely, causing lack of volume and underinflation.
Fracture. There may be a fracture of the implant, and it is more likely to occur with the malleable implants than the inflatable type, the authors concluded.