CT perfusion can be used to evaluate esophageal cancers with small tumor diameters that are not amenable to assessment with PET/CT, according to a new study by Turkish researchers presented at ECR 2014 earlier this month.
Esophageal cancer is one of the most common gastrointestinal malignancies with one of the worst prognoses, and its early diagnosis is of utmost importance, noted Dr. Mecit Kantarci, from the department of radiology at Ataturk University, during his presentation. CT, endoscopic ultrasound, and PET/CT are used in combination for early diagnosis and staging.
CT perfusion uses various parameters such as blood flow, blood volume, mean transit time, and permeability to demonstrate angiogenesis in tumor tissues and to assess microcircular changes noninvasively and quantitatively, he explained. Angiogenesis is important to the progression and aggressiveness of solid tumors, including esophageal cancer, he told AuntMinnie.com.
"CT perfusion has been used to assess vascularity within tumors in vivo," he said. "It is also possible with CT perfusion to accomplish a quantitative assessment using blood volume, blood flow, and permeability in tumors."
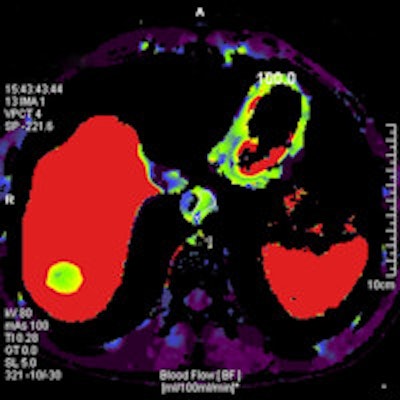
 A 68-year-old man with an 8-mm distal esophageal mass with biopsy-proven squamous cell carcinoma. On coronal PET, axial PET, and axial fused PET/CT images (above), the primary tumor demonstrates no significant FDG uptake. Axial CT image shows esophageal mass at the same level. In the same patient, functional perfusion maps of blood volume, blood flow, and permeability surface (below) reveal the intratumoral perfusion distribution. CT perfusion values for blood volume (left), blood flow (right), and permeability surface (bottom) were 9.62 mL/100 mL, 86.67 mL/100 mL/min, and 12.65 mL/100 mL/min, respectively. All images courtesy of Dr. Mecit Kantarci.
A 68-year-old man with an 8-mm distal esophageal mass with biopsy-proven squamous cell carcinoma. On coronal PET, axial PET, and axial fused PET/CT images (above), the primary tumor demonstrates no significant FDG uptake. Axial CT image shows esophageal mass at the same level. In the same patient, functional perfusion maps of blood volume, blood flow, and permeability surface (below) reveal the intratumoral perfusion distribution. CT perfusion values for blood volume (left), blood flow (right), and permeability surface (bottom) were 9.62 mL/100 mL, 86.67 mL/100 mL/min, and 12.65 mL/100 mL/min, respectively. All images courtesy of Dr. Mecit Kantarci.

CT perfusion could be preferred for assessing tumor angiogenesis because of its shorter examination time and its utility for quantitative assessment, he said. Therefore, the group developed a research protocol comparing CT perfusion and PET/CT for staging esophageal cancer.
Specifically, Kantarci and colleagues examined the correlation between CT perfusion parameters and glucose metabolism as assessed by whole-body PET/CT and maximum standardized uptake values (SUVmax).
The study included 31 patients (19 men, 12 women; mean age, 59) who underwent FDG-PET/CT for esophageal cancer staging and also had CT perfusion and thoracoabdominal CT with contrast for esophageal masses. Eight of the patients had adenocarcinoma and 23 had squamous cell carcinoma. The study was conducted between May 2012 and November 2013.
CT perfusion exams included the affected area of the esophagus, and multiple scans were obtained. The calculated average effective radiation dose for the perfusion scans was approximately 9 mSv, and all CT perfusion examinations were performed using a second-generation 256-slice CT scanner.
Based on the CT perfusion and PET/CT images, the authors divided the esophageal tumors into three groups depending on tumor diameter: 5-15 mm (48%), 15-25 mm (32%), and 25-35 mm (19%).
CT perfusion parameters of blood volume, blood flow, and permeability surface were compared with SUVmax generated from PET, and tumor diagnosis was confirmed histopathologically in all patients. Correlations between tumor grade, pathological cell types, and SUVmax and CT perfusion parameters were assessed.
 Dr. Mecit Kantarci from Ataturk University.
Dr. Mecit Kantarci from Ataturk University.
Key results are as follows:
- In all stages, no significant difference was found between CT perfusion and SUVmax values in esophageal cancers with varying histological types and tumor diameters.
- There was no significant difference between CT perfusion parameters in stage I, II, and III esophageal cancers. However, there was a significant difference between stage IV and the other stages with respect to blood-flow values.
- CT perfusion parameters were slightly higher in patients with adenocarcinoma than in those with squamous cell carcinoma.
- For stage I disease, there was no measurable FDG uptake in four patients with tumors 6- to 12-mm in diameter. However, CT perfusion values were measured in all cases.
Kantarci pointed out that the study had some limitations, such as a small sample size and the lack of a patient group with benign conditions. Also, CT perfusion involves a relatively high radiation dose, but dose reduction protocols can be used to limit exposure, as was done in the current study.
The study found good correlation between perfusion CT parameters and SUVmax values, but one of its most important findings was the significant difference between stage IV and other stages with respect to blood-flow values on the perfusion CT scans, according to Kantarci.
"I think perfusion CT has some advantages compared with F-18 FDG PET/CT, according to our study findings," Kantarci said.
The results can be of benefit to radiologists if they want to quantitatively evaluate tumor vascularity during staging and while examining response to therapy, he noted.
"The small tumors not detectable on PET/CT may be visible on CT perfusion," Kantarci concluded. "If there are presences of clinical suspicion and PET/CT findings are normal, CT perfusion imaging can be added to routine imaging examinations."



















