LIVERPOOL, U.K. - As cardiac CT services are accessed by an ever wider range of referrers, ongoing education is needed to ensure appropriate use, and simple guidelines can achieve this effectively, a leading group of researchers told attendees at this week's U.K. Radiological Conference (UKRC 2013).
"Our CT coronary angiography service was previously receiving unacceptably high rates of inappropriate referrals," noted Dr. Carl Roobottom and colleagues from the departments of cardiology and radiology at Derriford Hospital in Plymouth, U.K. "We identified patient-related factors contributing to nondiagnosis, assessable at the point of referral, and highlight these to our referrers with simple, educational guidelines. Our service has since been made available to noncardiologists."
The experience and confidence of reporters, along with improvements in technology, are likely to be important, but the group suggested the quality of the referral is still vital. Where CT is unsuccessful, patient factors -- such as heart rate or rhythm, and inability to breath-hold -- remain common.
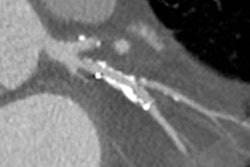
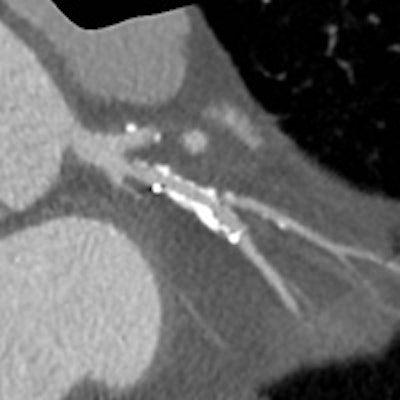
 Comparison images demonstrating how high-definition CTA improved reporting accuracy. The case is of a 49-year-old man with previous stent to the circumflex artery with recurrent pain. New scanner technology allows the use of CTCA in patients with known existing heart disease. This is not possible with a conventional CT scanner. This means the interventional cardiologist has all the required information to plan the subsequent intervention. Top left image shows a stent in the circumflex artery but no stenosis. Bottom left shows an occluded right coronary. Top middle also is of the circumflex but demonstrates how the use of the Discovery CT750 HD scanner (GE Healthcare) allows clear visualization of the short stenosis, despite the stent and high level of calcium in the arteries. Top right is a conventional left coronary angiogram confirming the CT findings. Bottom right is the right coronary angiogram confirming findings. All images courtesy of Dr. Carl Roobottom.
Comparison images demonstrating how high-definition CTA improved reporting accuracy. The case is of a 49-year-old man with previous stent to the circumflex artery with recurrent pain. New scanner technology allows the use of CTCA in patients with known existing heart disease. This is not possible with a conventional CT scanner. This means the interventional cardiologist has all the required information to plan the subsequent intervention. Top left image shows a stent in the circumflex artery but no stenosis. Bottom left shows an occluded right coronary. Top middle also is of the circumflex but demonstrates how the use of the Discovery CT750 HD scanner (GE Healthcare) allows clear visualization of the short stenosis, despite the stent and high level of calcium in the arteries. Top right is a conventional left coronary angiogram confirming the CT findings. Bottom right is the right coronary angiogram confirming findings. All images courtesy of Dr. Carl Roobottom.Having conducted an audit of their service for rate and cause of nondiagnosis in 2009, the Plymouth researchers decided to carry out a reaudit. All attendees for coronary CTA (CCTA) examinations for the investigation of coronary artery disease during a three-month period were reviewed. The analysis included 329 patients, and the cohort was similar to the original one, although it was older (59 versus 61 years) and with higher body mass indices.
In the recent audit, CCTA was not attempted in 20 patients. Overall, 13% were not attempted or not diagnostic, compared with 18.2% in 2009. The reasons for nondiagnosis were similar to those before: 57% due to heart rate and rhythm, and 36% unable to breath-hold. The nondiagnostic rate in patients referred by clinicians who had received the team's educational guidelines was 8% compared with 19% in those who had not. The rate for cardiologists was 10.6%, compared with 18.3% for other referrers.
The referral guidelines explain that CCTA is not appropriate for patients who are unable to lie flat and who cannot hold their breath for 15 seconds. They indicate that the patients who have the best chance of undergoing a useful scan are those with a resting heart rate of less than 65 beats per minute (bpm), or a resting heart rate of less than 75 and no contraindications to intravenous beta-blockers.
The outcome has been a significant improvement in the rate of nondiagnosis, according to Roobottom and colleagues. There has been a lower rate of nondiagnosis in those referred from clinicians who received the basic referral guidelines, as well as a lower rate of nondiagnosis in cardiologists compared with other referrers, they reported.