The seemingly irresistible proliferation of postmortem CT (PMCT) is continuing apace. The technique is already thriving in Denmark, Sweden, Switzerland, the U.K., the U.S., and Australia, and now a major study from France -- thought to be the nation's first on postmortem CT -- has produced a positive outcome.
"PMCT should be considered a very useful supplementary tool for forensic autopsy because imaging can detect small injuries that may be missed by traditional autopsy," noted Dr. Isabelle Le Blanc-Louvry, from the department of forensic medicine at Rouen University Hospital in France. "Because concordance between the findings of both radiologists was almost perfect or substantial, particularly in traumatic cases, autopsy could be avoided in these cases, except in cases of homicide."
This procedure is objective and rapid, and the resultant data are easy to store for future reference, she stated in the July edition of European Radiology. More modern CT systems provide greater anatomical scope, and CT can usually determine the cause of most deaths following trauma, although prospective studies are required to establish an algorithm for forensic CT.
The main aim of the French study was to determine the concordance between PMCT and autopsy in detecting traumatic or nontraumatic lesions according to the different anatomical regions. Secondary aims were to determine the efficacy of PMCT in showing lethal lesions proved by autopsy, as well to establish the interobserver agreement between the two radiologists.
Le Blanc-Louvry and her colleagues evaluated 236 PMCT scans performed from January 2006 to August 2011 at Rouen before external examination and autopsy (159 male and 77 female cadavers; age range 20 weeks to 78 years; mean age 42 years). The context of death was a traumatic event (other than gunshot or stab wounds) in 62 cadavers, and gunshot wounds, stab wounds, hanging, asphyxia other than hanging, drowning, and carbonization in 26, 17, 11, 11, 22, and 21 cadavers, respectively. In 66 cadavers, either nontraumatic lesions were observed or no lesions were detected. The mean delay between declaration of death and imaging was 6 ± 3 days, and that between PMCT and autopsy was 18 ± 1 hours.
All PMCTs were performed the day before autopsy. The examinations were performed on a 16-slice system (Light Speed Ultra unit, GE Healthcare) until December 2009 (92 cases, of which 62 were before autopsy), and afterward on a 64-slice unit (Discovery, GE Healthcare) (174 cases). An examination started with anteroposterior and lateral scout views, and typical parameters for the 64-detector-row unit were pitch 1.375:1, gantry rotation time 1.0 sec, tube voltage 120 kVp, current intensity 200 mA, field-of-view 50 cm for the entire body, including the head. The acquisition time was three minutes, and reconstruction takes about one minute more. Multiplanar software (Reformat, GE Healthcare) was used.
"Postmortem CT was assessed by a radiologist who was aware of the context of death," the authors wrote. "A second reading was performed by a second radiologist who was blinded to the results of the previous radiological analysis, but had knowledge of the autopsy findings. Both radiologists had previous experience in reading postmortem images. Detailed radiological evaluation was known to the two forensic pathologists at autopsy. However, only findings discovered during standard autopsy without performing additional dissection or particular techniques guided by PMCT (e.g., research of pneumothorax, gaseous embolus) were noticed."
Agreement between PMCT and autopsy was almost total in showing skull, basal skull, or hyoid bone fractures, whereas concordance between the two examinations was excellent in demonstrating facial, vertebral, and pelvic fractures and the number of fractures shown by PMCT was superior to that observed at autopsy. As for rib fractures, concordance between the two examinations was substantial and autopsy demonstrated more lesions than PMCT.
Discordance was observed in demonstrating intracranial injuries such as subdural hematomas, as well as pulmonary, vascular, or abdominal wounds. In these cases, the number of lesions demonstrated by PMCT was inferior to that determined by autopsy. Similarly, discordance was observed between the two examinations in detecting free air in anatomical cavities. In some cases, PMCT demonstrated findings that would not be shown by autopsy such as a muscular prosthesis inserted in a calf that allowed identification and a fracture of the dens of the axis.
"PMCT was very effective at demonstrating lethal lesions detected by autopsy in the context of craniofacial trauma as previously reported. In thoracic trauma, PMCT was inferior to autopsy in showing pulmonary, vascular, or heart wounds. PMCT was effective at detecting lethal gunshot wounds, but less effective after stab wounds, because tracks were more difficult to ascertain. In many cases, cause of death was only suspected because of indirect signs as in the case of effusions," the researchers noted.
Diagnosis of drowning is difficult to establish, even by autopsy, because only nonspecific anatomical findings are observed such as edema fluid in the nostrils, mouth, and airways, pulmonary edema and water in the lumen of the stomach, and because biological and histological samples are needed to confirm drowning. In charred bodies, no specific signs were found in our subjects and imaging of soot in the airways was never observed, they explained.
The study has limitations, the authors admitted. PMCT was not routinely performed at the beginning of the study because access to CT was limited, and pathologists were aware of the PMCT findings before the autopsy that allowed them to perform additional dissections guided by CT. Only lesions detected by standard autopsy without additional dissection were considered in the Rouen study. Also, the second radiologist had knowledge of the autopsy findings before image interpretation and was able to perform complementary reconstructions that increased CT performance.

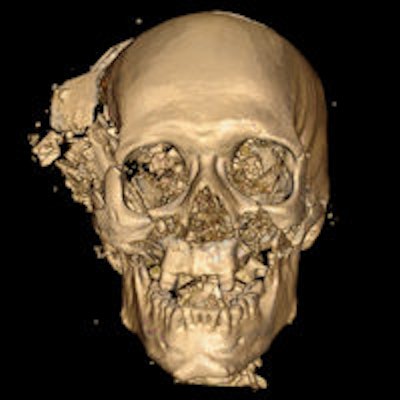
Note: The image above and on the home page is a volume-rendered 3D CT reconstruction of a homicidal death. Characteristic bony and metallic fragments are shown on the exit side of the skull, where the bullet caused a large loss of brain, leading to shattering of the skull. Image courtesy of Dr. Giuseppe Guglielmi; originally appeared in ECR Today 2013 newspaper.