Virtual autopsy can be defined as one that takes place without dissecting a body thanks to a combination of various imaging techniques, including MRI and CT. The idea of combining medical imaging with forensic investigations came from Dr. Gil Brogdon of the University of South Alabama (who died in March 2014), but the first thanatological use of the scanner comes from the Bern Institute of Forensic Medicine in Switzerland.
According to its creator, Dr. Michael Thali, the neologism "virtopsy" is a combination of virtual (from the Latin virtualis) and autopsy, and it means carrying out a virtual autopsy without recourse to the scalpel. It also involves improving the quality of data acquisition in forensic medicine (virtualis: usable, industrial, improved). Where the autopsy offers a "view of oneself," the virtopsy acts in a complementary way to give a "better view" and guide the autopsy.
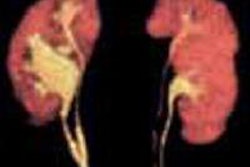
 Maximum intensity projection (MIP) late reconstruction of a postmortem angiography scan (third injection with body in dorsal decubitus).
Maximum intensity projection (MIP) late reconstruction of a postmortem angiography scan (third injection with body in dorsal decubitus).Advantages compared with autopsy
No destruction of evidence or indicators that might be damaged during a traditional autopsy within the framework of forensic autopsies
Option of "redoing" the virtual examination, which represents a considerable advantage; traditional autopsies can only be carried out correctly a single time. Images can thus be re-examined, modified, and reanalyzed as many times as is necessary, and there is no limit to the number of 2D and 3D reconstructions.
In medical autopsies, it overcomes religious and cultural barriers that forbid the "cutting up" of bodies.
Creation of digital files that may have a number of uses, such as being produced in court, permanent storage, electronic transfer of these images, and also for facilitating communication between professionals
There also exist advantages that are directly linked to the technique of the virtual autopsy:
It offers the option of gathering information from the whole body more quickly, and of studying those areas that are difficult or even impossible to access during traditional autopsies, and thus to carry out an autopsy directly on the areas of interest. This speed of operation could, for example, be used in rapid identification in cases of mass disaster.
This examination could be used in complex cases such as bioterrorism incidents because it would reduce the risk of contamination for pathologists and other medical personnel by avoiding the opening up and handling of a potentially contagious body. This particular context can be applied to all bodies that are infected or contaminated by toxins.
CT scanning also proves advantageous in the study of bodies that are in a state of putrefaction (recovered long after death, or after several days in the sea), carbonized, or in a skeletal state, especially with the aim of identifying the person and searching for projectiles and skeletal fractures forming part of injuries caused by a third party.
Practical limitations
One of the main limitations of the virtopsy is represented by the problem of the accessibility and availability of imaging equipment. Although Switzerland has dedicated machines, this is not necessarily the case in other countries. In addition, there is the problem linked to the extra cost represented by this whole series of examinations, all the more so because it remains a complement to existing examinations.
In France, around 7,000 autopsies are performed each year. Because the technical cost (not including the "intellectual" cost of the procedure) for a CT scan amounts to about 100 euros, and approximately double this for an MRI, the systematic use of these examinations would therefore constitute an additional cost to that of autopsies.
 From left to right: Christophe Bartoli (forensic medical examiner), Mathieu Coulange (hyperbaric doctor), Frédéric Cohen (radiologist), Pierre-Eloi Laurent (radiologist), Marianne Jolibert (radiologist), Guillaume Gorincour (radiologist), Marie-Dominique Piercecchi-Marti (forensic medical examiner), and Jean-Michel Bartoli (radiologist).
From left to right: Christophe Bartoli (forensic medical examiner), Mathieu Coulange (hyperbaric doctor), Frédéric Cohen (radiologist), Pierre-Eloi Laurent (radiologist), Marianne Jolibert (radiologist), Guillaume Gorincour (radiologist), Marie-Dominique Piercecchi-Marti (forensic medical examiner), and Jean-Michel Bartoli (radiologist).Prospects
Based on technical, scientific, and organizational experience in this area since 2008, we envisage an "ideal" theoretical way of functioning, which could allow these new methods to deliver their full potential, for the benefit of patients, research, and prevention.
This way of functioning would be based on multidisciplinary centers bringing together forensic medical examiners, radiologists, members of the police and their forensic departments, ballistics specialists, forensic scientists and toxicologists, experts in identification, imaging and animation engineers and technicians, and also legal experts, philosophers, sociologists, ethicists, etc.
These centers would have to be under the control of both a university body and a hospital, and also work closely with higher authorities such as Interpol on the problems of identifying victims. They would have to possess all the techniques necessary for optimum functioning and scientific development:
- 3D imaging of the surface of the body (photogrammetry)
- CT system and postmortem angiography machine
- MRI and MR spectroscopy
- Micro-MRI and micro-CT
- Equipment for imaging-guided percutaneous biopsies
- Amalgamation of surface and radiological data
- Conventional autopsy
The mission of these centers would be to continue the work of correlating "virtual" data and data from autopsies in order to come to a conclusion on their respective roles and limitations. They would also be tasked with promoting training and research in the forensic and medical-scientific fields, on a multidisciplinary basis.
Pierre-Eloi Laurent, Damien Ariey-Bonnet, Vincent Vidal, and Guillaume Gorincour work in the Laboratory of Interventional and Experimental Imaging at Aix-Marseille University, France. Christophe Bartoli and Marie-Dominique Piercecchi-Marti are based in the department of forensic medicine at Hôpital de la Timone, Marseille. The authors acknowledge the help of the medical and paramedic team, in particular Anthony Garbino and Laura Martinez Gongora, medical imaging technicians.
Editor's note: This is an edited translation of an article published in French on 19 October 2014 by the le Quotidien des JFR (Journées Françaises de Radiologie Diagnostique et Interventionnelle), the daily newspaper of the French national congress of radiology. Translation by Syntacta Translation & Interpreting.