The automated breast volume scanner (ABVS) is a promising diagnostic method with a good interobserver reliability, and it can overcome the limitations of handheld breast ultrasound (HHUS), German researchers have found in a new study.
Handheld ultrasound is an important instrument in complementary breast imaging, and is an accepted means of assessing suspicious lesions of the breast. It is often used in conjunction with breast cancer screening of asymptomatic women, especially those with dense breasts, but it lacks standardization and reproducibility, plus it takes time. ABVS was developed to combat these issues.
 Dr. Michael Golatta.
Dr. Michael Golatta.
ABVS combines automation and 3D scanning. The German researchers used the Acuson S2000 ABVS system (Siemens Healthcare), which allows an automated assessment of a complete 3D breast volume by a technician and provides the possibility of an evaluation of the reconstructed pictures by various physicians independent of time and location (European Journal of Radiology, 28 March 2013).
Dr. Michael Golatta, from the University Breast Unit at Heidelberg University Hospital, and colleagues analyzed the interobserver reliability between six different physicians evaluating the ABVS examinations breast wise and the agreement of ABVS results with handheld ultrasound, mammography, and histology results of according lesions.
All 42 study participants received an ABVS examination in addition to the conventional breast diagnostic workup. Twenty-five breasts (30%) showed at least one lesion. The scans were interpreted by six breast diagnostic specialists blinded to results of breast imaging and medical history. Thirty-two lesions received histological workup; 20 cancers were detected.
Based on BI-RADS, specialists agreed on 63 cases (75%); this number improved to 98% when dichotomizing the interpretation in benign (BI-RADS 1, 2) and suspicious (BI-RADS 4, 5) lesions. For more specific results, including sensitivities, specificities, positive predictive values (PPV), and negative predictive values (NPV), see the table below.
| Sensitivity | Specificity | PPV | NPV | False-positive rate | False-negative rate | |
| ABVS (mean all 6 raters; best value; worst value) | 82% (75/90%) | 68% (58/83%) | 81% (75/89%) | 69% (58/80%) | 12% (6/16%) | 12% (6.16%) |
| Handheld US | (100%)* | (25%)* | 69% | 100% | 28% | 0% |
| Mammography | (90%)* | (42%)* | 72% | 71% | 29% | 6% |
Source: Dr. Michael Golatta et al.
"Agreement of ABVS examination to HHUS, mammography, and pathology was fair to substantial depending on the specific analysis," the authors noted. "To our knowledge this is the first comprehensive report on ABVS interobserver reliability including a large proportion of symptomatic cases with information on histological results after biopsy."
ABVS might be a promising tool to overcome the lack of standardization and reproducibility of handheld ultrasound because 3D volumes of the whole breast allows the reconstruction of different views independent of the time and location of the actual examination, they added.
"From a methodological point of view, this is a very important basis to be able to develop and improve this system further," Golatta and colleagues wrote.
In addition to the good reproducibility and the agreement within different examiners, the possibility of missing a lesion should be less probable because volume data of the whole breast is available and can be evaluated by the examiner; this should result in high sensitivity and probably lower specificity, they added.
ABVS agreement with handheld ultrasound interpretation is fair compared with BI-RADS scores and is substantial when compared with dichotomized scores.
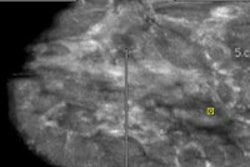
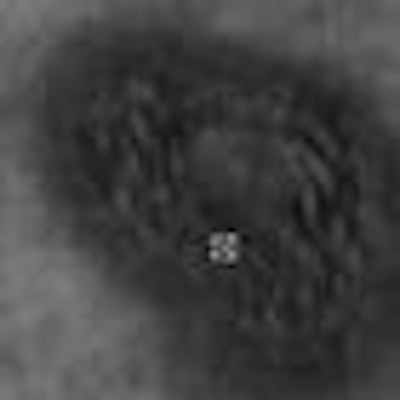
 Automated breast volume scan acquired with the Acuson S2000 ABVS1 machine. The skin line submillimeter image shows the coronal view of the breast, which is not available using conventional, handheld ultrasound. Image courtesy of Siemens Healthcare.
Automated breast volume scan acquired with the Acuson S2000 ABVS1 machine. The skin line submillimeter image shows the coronal view of the breast, which is not available using conventional, handheld ultrasound. Image courtesy of Siemens Healthcare.Limitations of the study include the following:
- The study had an explorative design.
- The examiner knew the clinical situation (scars, lumps, history of the patient, etc.) when performing the handheld ultrasound, which led to a nonblinded interpretation of the ultrasound findings.
- The results of mammography were available on the handheld ultrasound examination and interpretation, which was not the situation when interpreting the ABVS exams; the interpretations were blinded to simulate a screening situation.
"Nevertheless, we compared the ABVS with the HHUS results knowing that ABVS could actually perform even better, when having the clinical information," they wrote. "All the more, it is interesting that agreement rates and specificity is in an acceptable range for a new, experimental diagnostic method."
The relatively high false-negative rate of 12% is the most critical finding of the study, and has to be improved before ABVS can be proposed as a screening instrument, they concluded.
Study disclosure
Dr. Golatta received payment for lectures from Siemens Ultrasound.