Adding digital breast tomosynthesis (DBT) to mammography increases the accuracy for detecting soft-tissue mammographic abnormalities, whether DBT is compared with film-screen mammography alone or film-screen mammography plus full-field digital mammography (FFDM), U.K. researchers have reported.
While mammography is the current standard of care for breast cancer screening, it also has its limitations, namely anatomical noise from the superimposition of normal structures, meaning a tumor may be completely or partially obscured. Normal structures may produce an appearance with conventional 2D mammography that seems suspicious and leads to a recall.
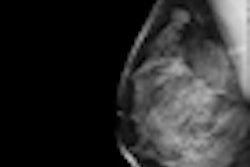
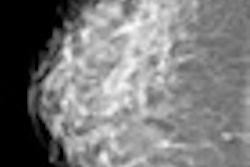
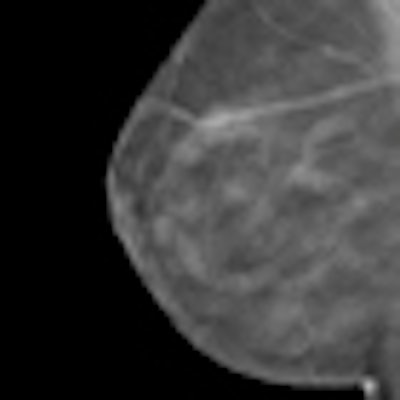
DBT improves the accuracy of mammography by enabling the reader to view x-ray images of the breast tissue as a series of thin reconstructed sections, which overcomes the problem of overlying tissues on conventional 2D images, according to a research team led by Dr. Michael Michell, a consultant radiologist at King's College Hospital in London.
"Some data have shown an improvement in specificity and BI-RADS classification of lesions using DBT alone or in combination with FFDM," Michell wrote in an article in press from Clinical Radiology on 22 May. "However, there remains some uncertainty about whether and how DBT should be used in routine screening, in the assessment and diagnostic workup of mammographically detected abnormalities found in routine screening, and in women presenting with breast symptoms."
The researchers sought to examine the effect FFDM and DBT had on the diagnostic accuracy of mammography in a population of women recalled following film-screen mammography alone. From January 2009 to July 2010, 738 women participated. They underwent bilateral two-view mediolateral oblique and craniocaudal FFDM and DBT within a single compression episode for each projection using a FFDM unit with tomosynthesis capability (Selenia Dimensions, Hologic).
The unblinded readers found 204 malignant lesions, 286 benign lesions, and 269 normal lesions. The researchers assessed diagnostic accuracy by using receiving operating characteristics (ROC) and measurement of the area under the curve (AUC).
DBT significantly improved the accuracy compared with film-screen mammography alone and FFDM with film-screen mammography combined. For film-screen mammography alone, the AUC was 0.7882 ± 0.0198, for FFDM with film-screen mammography combined the AUC was 0.8949 ± 0.0124, and with the addition of DBT the AUC was 0.9671 ± 0.0050, the researchers found.
Computed values for absolute sensitivity, specificity, positive predictive value
(PPV), and negative predictive value (NPV) of histology-proven malignant
lesions
|
||||||||||||||||||
| aAbsolute sensitivity = M5 counted as positive. bComplete sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) = M3 + M4 + M5 counted as positive. |
||||||||||||||||||
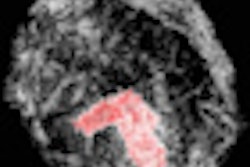
Of the 204 cancers, 34.3% were classified as malignant on film-screen mammography; FFDM bumped up the percentage to 39.7%, and with FFDM and DBT the percentage was 58.3%, the authors found. DBT resulted in fewer malignant lesions being classified as M3/M4 compared with film-screen mammography and FFDM combined. Additionally, six of the 204 cancers were only visualized on DBT.
DBT also classified more normal/benign cases as M1/M2 (74.2%), compared with film-screen mammography alone (3.78%) and FFDM with film-screen mammography combined (50.9%). In soft-tissue lesions, the researchers found a significant difference in accuracy between FFDM with film-screen mammography combined and the addition of DBT -- AUC was 0.9201 ± 0.0133 and 0.9905 ± 0.0024. This was to be expected from the reduction in anatomical noise. However, regarding microcalcification, they found no significant difference between the two imaging techniques.
"In this study of women recalled for further assessment following routine screening, FFDM was more accurate than film-screen mammography," Michell noted. "This is consistent with the findings of trials comparing the accuracy of film-screen mammography and FFDM. The addition of DBT, however, showed a significant improvement in accuracy compared to both film-screen mammography alone and film-screen mammography and FFDM combined."
The results from this study, as well as others, have implications for both screening and diagnostic practice in the future, the authors stated.
"DBT may increase the efficiency and effectiveness of screening through improvement in both specificity and sensitivity," they wrote. "Better visualization of normal and benign features may improve the ability of the film reader to confidently diagnose cases without malignancy and thereby reduce the recall rate, with savings in resources for the healthcare system, and fewer women suffering the anxiety and inconvenience associated with recall."
Improved visualization of abnormal features may possibly also boost detection of small cancers with subtle signs and decrease the false-negative interval cancer rate, the researchers added.
The potential improvements in specificity and sensitivity, as well as cost-effectiveness, need to be addressed in large-scale trials.
"Further studies are required to assess the added value of DBT in the diagnostic workup and local staging of malignancy in the context of the full range of current techniques, including ultrasound, magnification and spot compression mammography, and MRI," Michell wrote.