Shear-wave elastography (SWE) is highly reproducible for assessing elastographic features of breast masses, an eminent ultrasound researcher has found. Additionally, shear wave elastography is at least as consistent as BI-RADS ultrasound B-mode features, which could aid in classifying masses.
Breast ultrasound is well-known as a valuable adjunct to mammography, but it has low specificity. Elastography may be able to improve patient management for masses with a low index of suspicion on B-mode ultrasound. The problem is it can be difficult to capture the same information across acquisitions or users as each elastography method varies, depending on the manufacturer.
"For any elastographic approach to become widely accepted, consistent image generation and interpretation must be demonstrated," wrote lead author Dr. David Cosgrove, emeritus professor in the imaging sciences department at London's Imperial College, and colleagues in a study published online in European Radiology (30 December 2011). "Therefore, the purpose of this study was to evaluate the intra- and interobserver reproducibility of shear-wave elastography for breast masses."
 BE1 SWE of a benign mass showing the QBox. This palpable lesion was scored as BI-RADS 4a by the investigator, suggesting it carried a risk of malignancy, but it was soft on SWE with very low Emax values (20 kPa), suggesting that it was benign. Histology of the biopsy specimen revealed a fibroadenoma. Image courtesy of Dr. Christophe Tourasse, Hôpital Louis Mermoz in Lyon, France.
BE1 SWE of a benign mass showing the QBox. This palpable lesion was scored as BI-RADS 4a by the investigator, suggesting it carried a risk of malignancy, but it was soft on SWE with very low Emax values (20 kPa), suggesting that it was benign. Histology of the biopsy specimen revealed a fibroadenoma. Image courtesy of Dr. Christophe Tourasse, Hôpital Louis Mermoz in Lyon, France.Shear-wave elastography is a technique in which an acoustic pressure wave induces slow-moving lateral waves within the tissue, and the speed of propagation of the shear wave is proportional to the square root of the tissue's elastic modulus. Shear waves travel slower in softer tissue and faster in stiffer tissue. Small changes in velocity occur when the waves pass through tissues of varying stiffness, which is then mapped to create an image. SWE features such as the minimum, mean, and maximum elasticity in a region of interest also can be measured.
In Cosgrove's study, each of the investigators obtained three consecutive SWE images (Aixplorer, SuperSonic Imagine) of 758 masses visible on ultrasound. Of those, 19% were malignant. The reliability of quantitative measurements was assessed by intraclass correlation coefficients. In addition, a blinded observer reviewed images to determine agreement on features for the interobserver reproducibility. Weighted kappa was used to assess the agreement of qualitative elastographic features between observers.
Of the women screened, the average age was 50 and the average mass size was 13 mm. Qualitatively, SWE images were at least reasonably similar for 666 out of 758 (87.9%) masses. Intraclass correlation (ICC) for SWE diameter, area, and perimeter was almost perfect (ICC ≥ 0.94), according to the researchers. Intraobserver reliability for maximum and mean elasticity was almost perfect (ICC = 0.84 and 0.87, respectively). Intraobserver reliability for the ratio of mass-to-fat elasticity was substantial (ICC = 0.77). Interobserver agreement was moderate for SWE homogeneity (κ = 0.57), substantial for qualitative color assessment of maximum elasticity (κ = 0.66), fair for SWE shape (κ = 0.40), fair for B-mode mass margins (κ = 0.38), and moderate for B-mode mass shape (κ = 0.58), orientation (κ = 0.53), and BI-RADS assessment (κ = 0.59).
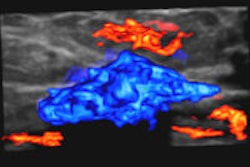
 BE1 SWE of a heterogeneous lesion that proved to be malignant. This impalpable lesion was found at mammography in a 66-year-old patient. On B-mode, the investigator scored the lesion as BI-RADS 4a. The heterogeneous pattern on the elasticity map confirmed the level of suspicion. The pathological outcome was a mixture of invasive and in situ ductal carcinoma. Image courtesy of Dr. Fritz KW Schäfer, University Hospital, Schleswig-Holstein in Kiel, Germany.
BE1 SWE of a heterogeneous lesion that proved to be malignant. This impalpable lesion was found at mammography in a 66-year-old patient. On B-mode, the investigator scored the lesion as BI-RADS 4a. The heterogeneous pattern on the elasticity map confirmed the level of suspicion. The pathological outcome was a mixture of invasive and in situ ductal carcinoma. Image courtesy of Dr. Fritz KW Schäfer, University Hospital, Schleswig-Holstein in Kiel, Germany.The heterogeneity of the SWE stiffness was moderately predictive of malignancy in the full set of masses with 70.6% of heterogeneous masses malignant, compared with 4.3% of homogenous masses in a population with 30.8% prevalence of malignancy.
"In both intra- and interobserver comparisons, breast SWE was highly reproducible, as might be expected of a technique that minimizes operator input," the authors wrote. "This underlies its value in improving the BI-RADS classification of breast masses and suggests that SWE should be useful for serial comparative studies. It should also aid in standardizing reporting of the elasticity of breast masses."
The investigators may have been confused when assessing the "similarity" of SWE images because three acquisitions -- each showing heterogeneous stiff and soft areas in a given lesion and its surrounding tissue -- were similar to each other, but were sometimes rated as "dissimilar" by investigators, noted Cosgrove, who retired in 2004 but is still a part-time consultant in radiology at Hammersmith Hospital in London.
 Breast ultrasound is a valuable adjunct to mammography, but it has low specificity. Elastography may improve patient management for masses with a low index of suspicion on B-mode ultrasound.
Breast ultrasound is a valuable adjunct to mammography, but it has low specificity. Elastography may improve patient management for masses with a low index of suspicion on B-mode ultrasound.
Despite this, the quantitative assessment of maximum and median elasticity was highly reliable across multiple SWE acquisitions, the authors found. "For clinical use, we suggest that orthogonal SWE acquisitions be performed, with clinical management of the lesion based on its most suspicious SWE features, together with its B-mode features. A lesion that is highly suspicious on B-mode should still be biopsied, regardless of its SWE appearance."
The researchers point out the method for comparing different elastographic images could markedly affect the intraobserver reproducibility reported across the literature. For instance, if one person collects the images for subsequent repeated scoring by one or more observers, it would always give more reproducible results than separate acquisitions as performed in this series. And reproducibility is of course important for the widespread adoption of any imaging technique.
"Consistent image generation is critical for serial studies of masses, for example, follow-up of probably benign masses, or to monitor the response of breast carcinomas to neoadjuvant chemotherapy, and the reliability of SWE could be helpful in these clinical situations," the authors wrote. "Standardizing the color display across elastography systems so that, for example, soft tissues are consistently blue and stiff tissues consistently red, would avoid confusion in centers with multiple different systems, or on receipt of images from outside facilities, and should urgently be addressed."
Limitations
The limitations of the study included the following:
- 174 masses (included 141 malignancies) were excluded from reproducibility analysis because the SWE values exceeded the (default) 7.7 m/sec upper limit that was preset for the scale.
- Difficulties and errors in the placement of the Q-box could have had a negative effect on the reproducibility of the measurements.
- The blinded second read was retrospective, with only two static B-mode images and one SWE image available for each mass. (Ideally, a prospective interobserver comparison would use real-time image acquisition.)
- Conventional ultrasound in 2D with resulting differences in slice selection across acquisitions and reliability of SWE imaging in all planes were not compared.
It should be noted the authors received consulting fees, and in Cosgrove's case, travel expenses, from SuperSonic Imagine.
The study was carried out in the U.S. and Europe on a prototype ultrasound system of the Aixplorer, under International Review Board (IRB) approval. The Aixplorer system legally available for sale in the U.S. does not include the quantification tool.