Computer-aided detection (CAD) is making an elusive breast abnormality a little clearer by highlighting the calcifications that often surround it. A new study sheds light on the detection of lobular carcinoma in situ (LCIS): clumps of abnormal cells in the breast lobules that aren't actually breast cancer but often precede or accompany it.
The nature of the association between LCIS and breast cancer isn't entirely clear, and, consequently, the management of LCIS remains controversial. Should LCIS be considered a simple incidental finding -- or removed whenever it's found?
In any case, mammography is generally blind to LCIS. But the lesions are often adjacent to calcifications, allowing CAD systems to nail LCIS most of the time, researchers concluded.
"LCIS isn't associated with any specific mammographic or clinical features, but it can be identified in near proximity to microcalcifications by needle or excisional biopsy," said Stamatia Destounis, MD, from Elizabeth Wende Breast Care in Rochester, NY. "Especially with vacuum-needle biopsies, we're able to extract large samples in a small amount of time in the vicinity of whatever we're targeting."
Lobular carcinomas are often discovered as incidental findings, typically after an abnormal mammography finding on subsequent needle biopsy, Destounis said in a presentation at the June Computer Assisted Radiology and Surgery (CARS) meeting in Geneva.
"CAD is a helpful tool for radiologists at identifying lesions that may require further attention, so the purpose of our review was to evaluate the performance of CAD on calcifications in patients with LCIS," she said. R2 (Hologic, Bedford, MA) and iCAD (Nashua, NH) CAD applications are used by Elizabeth Wende's mammographers in the facility, which takes a multimodality approach -- full-field digital mammography, MRI, and ultrasound -- to screening women for breast cancer.
Elizabeth Wende's retrospective review covered all cases of LCIS diagnosed between 2000 and 2009. In that time, Destounis and her colleagues recorded data for 57 patients with 58 diagnoses of LCIS (one patient had two lesions) at needle core biopsy. They logged data on patient demographics and presentation, in addition to the following information:
- Breast density
- Lesion type and location
- Lesion palpability
- Number of CAD marks, if any
- Needle biopsy method, including needle size and pathology results
- Surgical pathology, type of surgery, and follow-up imaging
Among the 58 LCIS tumors, mammography alone detected 67% (n = 39) of the lesions, Destounis said. Seven percent (n = 4) of the LCIS lesions were detected on ultrasonography and were not detected by mammography, and 21% (n = 12) of lesions were detected by both mammography and ultrasonography, while three of the lesions were detected at MRI.
"We had to get rid of nine of the cases because we didn't have the original CAD markings available," leaving 49 cases for the analysis of CAD performance, Destounis said. Of these 49 cases, the patients' ages ranged from 40 to 93 years (average, 56 years).
 |
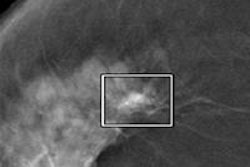
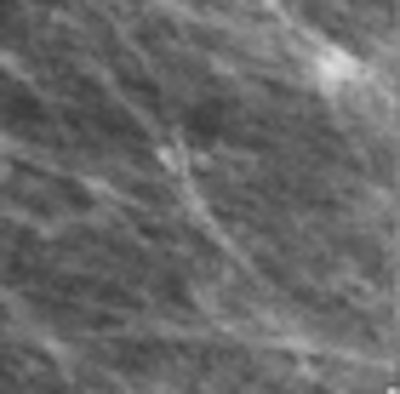
| Above, CAD missed the subtle calcification near LCIS while marking several other regions. CAD marked the LCIS lesion on both views in the patient shown below. Images courtesy of Stamatia Destounis, MD. |
 |
Needle core biopsy was performed on all 58 lesions, including 47 (81%) that were biopsied stereotactically, eight (14%) guided by ultrasound, and three (5%) guided by MRI.
Surgical excision was performed in 57 of the 58 lesions, as one patient with a prior LCIS chose imaging follow-up rather than surgery.
Pathology revealed 21 cancers (37%), 28 cases (49%) with atypia or high-risk findings, and eight lesions (14%) with benign findings. Twenty-eight of the patients who proceeded to surgery underwent subsequent additional surgery, including 18 patients for lumpectomy and 10 for mastectomy.
A total of 82% (n = 40) of lesions had pure calcium, or calcium associated with the main lesion, Destounis said. The following lesion types were observed:
- 32 calcifications
- 5 masses with calcium
- 6 masses
- 2 architectural distortions
- 2 architectural distortions with calcium
- 1 asymmetry
- 1 MRI enhancement with calcium
When LCIS lesions were associated with microcalcifications, CAD marked the calcifications 82.5% of the time, Destounis said.
"CAD appears to be helpful in the detection of LCIS, and in the high-risk lesions in our review had a considerable number of cases with associated calcium," Destounis said.
"There's a lot of controversy about LCIS, whether it should be surgically removed -- whether it's an incidental finding that you just happen to fall upon or invasive cancer when that's found," Destounis said. "But in our clinic, we remove LCIS every time we find it, because atypia such as [atypical ductal hyperplasia] or invasive lobular cancer or [ductal carcinoma in situ] are often found to be associated with LCIS," she said.
By Eric Barnes
AuntMinnie.com staff writer
August 20, 2010
Related Reading
Technology, not biology, makes for lower mammo performance, August 2, 2010
Double readers top CAD in finding breast tissue deformities, July 26, 2010
Follow-ups boost mammo use among insured low-income women, June 30, 2010
Mammography screening hard-hit by economic downturn, June 22, 2010
Ignoring breast CAD detections cuts sensitivity, October 23, 2009
Copyright © 2010 AuntMinnie.com