Clinical research has begun to suggest that fluorine-18 (F-18) FDG-PET and contrast-enhanced breast MRI can be powerful tools for diagnosis and treatment staging in women with suspected breast malignancy. But FDG-PET for these patients is limited by its variable sensitivity -- certain types of breast cancer have abnormally low FDG uptake. One solution is to add CT data to PET scans to improve the modality's sensitivity, specificity, and overall accuracy for detecting breast cancer.
Furthermore, does the accuracy of the technology continue to improve when the FDG-PET/CT scan is conducted at two time points rather than one? Studies suggest that breast malignancies show a gradual increase in standard uptake values (SUV) over time after FDG injection, implying that imaging again, after at least 30 minutes have passed, could make FDG-PET imaging of the breast more effective.
Dr. Massimo Imbriaco and colleagues at the Università degli Studi di Napoli Federico II in Naples, Italy, compared dual-time-point F-18 FDG-PET/CT performed with the patient in the prone position to contrast-enhanced MRI (American Journal of Roentgenology, November 2008, Vol. 191:5, pp. 1323-1330).
The study included 44 patients with 55 breast lesions. The women underwent two PET/CT scans (Discovery LS, GE Healthcare, Chalfont St. Giles, U.K.) and one breast MRI on a 1.5-tesla whole-body system (Gyroscan Intera, Philips Healthcare, Andover, MA). The team also calculated the average percentage of change in standard uptake values (Δ%SUVmax) for PET/CT between time point 1 and time point 2.
The PET exam consisted of a whole-body scan and a four-slice multidetector CT exam, followed by images of the breast with the patient in the prone position (time point 1). Three hours after this first time point acquisition, a second PET scan was performed (time point 2). Data from the PET/CT scans were analyzed on an image fusion workstation (Xeleris, GE Healthcare). The MRI exam was performed with a dedicated four-element sense-compatible breast surface coil.
Of the 55 lesions, 10 were benign and 45 were malignant. Of the malignant lesions, 38 were ductal carcinomas and seven were lobular carcinomas. The size of the breast tumors ranged from 7 mm to 30 mm; 35 lesions were larger than 10 mm, while the remaining 20 were smaller than 10 mm.
 |
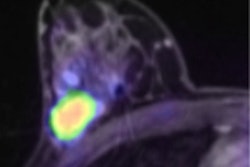
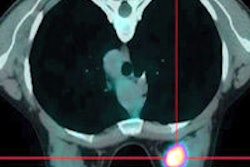
| Fifty-five-year-old woman with ductal infiltrating adenocarcinoma measuring 15 mm in maximum transverse diameter. Axial fused PET/CT images obtained with patient in prone position at time point 1 (above) and time point 2 (below) show corresponding standard uptake values. All images courtesy of the American Roentgen Ray Society. |
 |
 |
| Above, subtracted contrast-enhanced T1-weighted axial MR image shows focal area of intense F-18 FDG uptake and marked gadolinium enhancement in inferior inner quadrant of left breast. |
 |
| Thirty-two-year-old woman with ductal infiltrating adenocarcinoma measuring 18 mm in maximum transverse diameter. Axial fused PET/CT images obtained with patient in prone position at time point 1 (above) and time point 2 (below) show corresponding standard uptake values. |
 |
 |
| Above, subtracted contrast-enhanced T1-weighted axial MR image shows focal area of intense F-18 FDG uptake and marked gadolinium enhancement in superior inner quadrant of right breast. |
MRI proved 95% accurate, 98% sensitive, and 80% specific. For lesions smaller than 10 mm, MRI was 97% accurate; for those larger than 10 mm, it was 90% accurate. Dual-time-point PET/CT was accurate 84% of the time overall for lesions with an SUVmax greater than or equal to 2.5 or with a positive Δ%SUVmax. For lesions smaller than 10 mm, dual-time-point PET/CT's overall accuracy, sensitivity, and specificity were 89%, 88%, and 100%, respectively, versus single-time-point PET/CT, which attained 77%, 75%, and 100%, respectively.
Overall MRI and early and late PET results in 44 patients with final histopathologic diagnosis
|
||||||||||||||||
| Note for all tables: Data in parentheses are 95% confidence intervals. PET was performed with patient in prone position. Courtesy of the American Roentgen Ray Society.
|
MRI and early and late PET results in 35 malignant and benign lesions with a diameter > 10 mm
|
MRI and early and late PET results in 20 malignant and benign lesions with a diameter < 10 mm
|
On the PET/CT exams, malignant lesions showed an increase in FDG between time points 1 and 2, with a Δ%SUVmax of 11 ± 24.
Imbriaco's team concluded that dual-time-point imaging with acquisition in the prone position improves PET/CT accuracy in patients with suspected breast cancer over single-time-point PET/CT, but that the limited sensitivity of FDG-PET/CT, especially for lesions smaller than 10 mm, shows that the technology shouldn't be used as a routine imaging procedure for these patients. For lesions smaller than 10 mm, MRI shows higher sensitivity and should be preferred.
"Dual-time-point imaging can improve the sensitivity of PET, especially in mammographically dense breasts, which normally show increased FDG uptake," the authors wrote. "The application of dual-time-point imaging of the breast can improve overall accuracy of the technique by correctly identifying benign normal tissue and inflammatory lesions that at times may mimic cancer."
By Kate Madden Yee
AuntMinnie.com staff writer
November 18, 2008
Related Reading
MRI and FDG-PET/CT recommended for advanced breast cancer, April 4, 2008
PET/CT beats 3T MRI in whole-body primary tumor staging, March 10, 2008
FDG-PET/CT aids in radiation therapy planning, March 5, 2008
False positives a concern with FDG-PET/CT for head, neck tumors, January 31, 2008
PET/CT moves closer to diagnostic standard of care, March 1, 2007
Copyright © 2008 AuntMinnie.com