CHICAGO - In a head-to-head comparison of two closely watched modalities, low-dose dual-source coronary CT angiography (CTA) outperformed cardiac MR (CMR) in sensitivity, specificity, and negative predictive value (NPV). But 1.5-tesla CMR countered with better specificity and positive predictive value (PPV) compared to CT. Combining the modalities didn't improve results in the small but painstakingly performed study presented on Monday at the 2009 RSNA meeting.
The study was a combined effort between University Hospital Zurich in Switzerland and Massachusetts General Hospital in Boston, using conventional angiography results as the gold standard and referee in all cases.
"Conventional coronary angiography is the clinical standard of reference for coronary artery disease," said Dr. Olivio Donati from Zurich. "Prospectively, ECG-gated CT coronary angiography has proven to be a robust and accurate tool for significant coronary stenoses. Cardiac magnetic resonance provides indirect detection of CAD and has shown good diagnostic performance. Our study aimed to prospectively compare the diagnostic performance of CTA and cardiac MR as well as combinations thereof in a single patient cohort, taking coronary angiography as the standard of reference."
The researchers examined 43 consecutive patients (34 men, 9 women; mean age, 63 ± 9 years) with known or suspected coronary artery disease, who had been referred for elective coronary angiography, mostly presenting with chest pain.
All underwent invasive coronary angiography, followed by dual-source coronary CTA with prospective electrocardiography-gating, and accelerated 1.5-tesla cardiac MRI using a k-space and time broad-use linear acquisition technique. CT and MR studies were acquired on the same day. Stenoses were diagnosed indirectly in CMR by looking for perfusion defects.
Dual-source CT (Somatom Definition, Siemens Healthcare, Erlangen, Germany) was acquired using prospective ECG-gating at 70% of the RR interval, 2 x 64 x 0.6-mm slice acquisition, and 0.4-mm reconstruction increments, Donati said. 120 kV was used for patients with body mass index (BMI) of 25 or greater, with 100 kV used for the remaining patients.
A 1.5-tesla Intera CV MRI scanner (Philips Healthcare, Andover, MA) with a five-element cardiac synergy coil was used to acquire the MRI studies. First-pass perfusion imaging included:
- K-t BLAST (broad use linear acqusition speed-up technique)
- 11 interleaved training profiles
- k-t acceleration factor 5 to 3.7
- 40 consecutive cardiac cycles
- 2 x 2 x 10-mm3 (rec. 1.25 x 1.25 x 10-mm3) slices
To validate the results, the group analyzed a number of combinations, including low-dose CTA, adenosine stress-rest perfusion cardiac MR; late gadolinium enhancement (LGE), low-dose coronary CTA; and low-dose CTA combined with perfusion cardiac MR and LGE. Two highly experienced readers examined images in each modality.
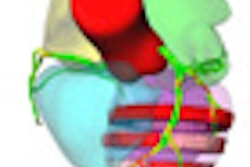
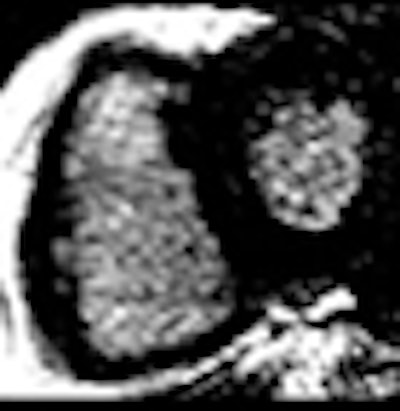
 |
| Results in one patient show a perfusion deficit in the intraseptal region. (CTCA = CT coronary angiography; ICA = invasive coronary angiography.) All images courtesy of Dr. Olivio Donati. |
According to the results, coronary angiography revealed greater than 50% diameter stenoses in 68 of 129 (57.7%) coronary arteries in 29 of 43 (70%) patients, Donati said.
In the patient-based analysis, sensitivity, specificity, NPV, and PPV of low-dose CTA for the detection of significant stenoses were 100%, 92.9%, 100%, and 96.7%, respectively. For perfusion cardiac MR and LGE combined, sensitivity, specificity, NPV, PPV, and accuracy were 89.7%, 100%, 82.4%, and 100%, respectively.
A per-vessel analysis showed the sensitivity and NPV of low-dose CTA to be significantly greater (p < 0.05) than both perfusion cardiac MR and LGE.


"Coronary CTA sometimes overrated the degree of stenosis," Donati said, and it was for this reason that none of the combinations of low-dose CTCA and perfusion cardiac MR improved the results.
"We took the good sensitivity from CTA, and unfortunately we also took the specificity from coronary CTA, because patients who were overrated with coronary CTA were thrown into the false-positive group" for the combined analyses, he said.
Donati concluded that CTA outperforms cardiac MR with regard to sensitivity and NPV, but cardiac MR is more specific and has a higher PPV than CTA, and combinations of the two exams didn't improve the diagnostic performance when compared to CTCA alone.
An audience member commented that patient selection and the readers' own thresholding biases were likely to play an outsized role in the results, considering the small cohort size. Absent more patients and more readers, receiver operator characteristics (ROC) analysis would likely help validate the results, the audience member said.
Another attendee said based on these conclusions, it wouldn't make a lot of sense to guide patients to hybrid modalities. Donati disagreed, stating that it's important to know which modality called the stenosis.
By Eric Barnes
AuntMinnie.com staff writer
December 1, 2009
Related Reading
CT-STAT trial finds CTA cheaper for solving chest pain riddles, November 19, 2009
CE-MRA helps plan treatment of patients with peripheral artery issues, November 10, 2009
CMS takes comments on MRA policy, October 9, 2009
Cardiac MR techniques improve myocardial assessment, June 15, 2009
Copyright © 2009 AuntMinnie.com