Cardiac CT has made great strides displacing conventional invasive coronary angiography, but its potential is still being tested, as new technologies are implemented and myriads of clinical trials get underway to boost understanding and improve their clinical utility.
A rapidly emerging technique is fractional flow reserve CT (FFR-CT), which offers new insights into the evaluation of coronary stenosis significance, according to Dr. Gorka Bastarrika, a cardiothoracic radiologist at Clinica Universidad de Navarra in Pamplona, Spain.
"The main advantage of FFR-CT is that it provides functional information of coronary stenosis severity, which is particularly important in intermediate lesions," he noted. "The addition of FFR-CT may increase the specificity and positive predictive value of CCTA [coronary CT angiography] and help reclassify false-positive patients as true negatives."
The technique also adds the benefit of obtaining functional information without added radiation, as opposed to myocardial CT perfusion, for example. It also has potential for planning and estimating the effect of coronary intervention before the procedure.
There are limitations, however. Bastarikka, a speaker at today's Special Focus session, said these include the fact that FFR-CT is very dependent on the image quality of CCTA. Accuracy of the results depends on adequate contrast opacification of the coronary vasculature and absence of artifacts. The coronary flow is based on mathematical algorithms being developed by industry. Supercomputational power is required for the analysis from proprietary software, and CCTA images need to be transmitted to the company for processing.
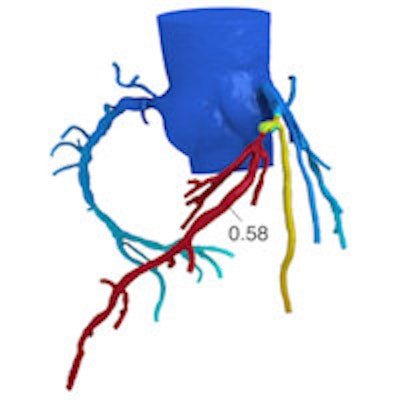
 The HeartFlow FFR-CT analysis is a noninvasive test that applies computational fluid dynamics to CT data to determine the extent that coronary artery obstructions are impacting blood flow to the heart. Here, a color-coded image from the HeartFlow analysis shows an artery with a 0.58 FFRCT value, indicating a lesion that may be functionally significant. Image courtesy of HeartFlow.
The HeartFlow FFR-CT analysis is a noninvasive test that applies computational fluid dynamics to CT data to determine the extent that coronary artery obstructions are impacting blood flow to the heart. Here, a color-coded image from the HeartFlow analysis shows an artery with a 0.58 FFRCT value, indicating a lesion that may be functionally significant. Image courtesy of HeartFlow.Although less expensive than conventional FPR, the cost of FFR-CT is set by the manufacturer, he explained. Several companies are currently developing software that can generate FFR data onsite, and when these products are approved for clinical use, the main hurdle for widespread adoption of this technology will be eliminated.
FFR-CT applies computation fluid-dynamic modeling to an anatomical model of the coronary artery tree segmented from CCTA. A mathematical model is created to establish coronary artery physiology. Blood flow is modeled using specific equations for fluid flow. Specifically, fractional flow reserve from CT enables calculation of rest and hyperemic pressure fields in coronary arteries.
Three large multicenter clinical trials (DISCOVER-FLOW, DeFACTO, and NXT) have validated the only commercially available technology (HeartFlow) against conventional FFR with encouraging results. In July 2011, European regulators approved the product for clinical use, but only a handful of hospitals in Europe are currently using the technology. The product received U.S. Food and Drug Administration clearance in November 2014.
Also, CT stress myocardial perfusion (CTP) has emerged as a promising method, which when combined with CCTA, can improve the evaluation of coronary artery stenosis in high-risk patients. Like FFR-CT, its use can help improve diagnostic accuracy by combining the anatomic aspect of CCTA with a physiologic assessment. The combined use of CCTA and stress CTP also has been shown to reduce the number of false positives. This may reduce the number of unnecessary invasive procedures and, in many cases, offers a less expensive alternative.
There are two approaches to stress CTP: static, in which images are acquired during a predefined single time point; and dynamic, in which images are acquired over a predetermined period of time to characterize the wash-in and wash-out of contrast medium in the myocardium. However, dynamic stress CTP is becoming the preferred choice for clinical routine due to the rapid progress in hardware and software for dose reduction, according to Dr. Kakuya Kitagawa, an assistant professor in the department of radiology at Mie University Hospital in Tsu City, Japan.
At today's session, he described state-of-the-art techniques for image acquisition and discussed the advantages and limitations of dynamic stress CTP and myocardial delayed enhancement (CTDE).
 A 61-year-old woman with atypical chest pain. Focal calcification in proximal left anterior descending (LAD) artery precluded assessment of degree of stenosis. Dynamic CT stress myocardial perfusion imaging showed reduced stress perfusion in the anteroseptal wall and apical wall, suggesting LAD stenosis. Invasive coronary angiography demonstrated high-grade stenosis with reduced FFR in the proximal LAD. Image courtesy of Dr. Kakuya Kitagawa.
A 61-year-old woman with atypical chest pain. Focal calcification in proximal left anterior descending (LAD) artery precluded assessment of degree of stenosis. Dynamic CT stress myocardial perfusion imaging showed reduced stress perfusion in the anteroseptal wall and apical wall, suggesting LAD stenosis. Invasive coronary angiography demonstrated high-grade stenosis with reduced FFR in the proximal LAD. Image courtesy of Dr. Kakuya Kitagawa.A key dilemma is whether stress CTP is ready for prime time.
"I think comprehensive CT combining dynamic CTP with quantitative analysis, CTA, and CTDE is already a powerful clinical tool. I would recommend our CT protocol to my family over MRI or SPECT if they have suspicious chest pain. But the environment to use CTP as clinical routine is not ready yet. We need more evidence on diagnostic accuracy and prognostic value. And of course, availability is also very important. The use of the technology in Japan, for example, is still limited to a few academic hospitals," he said.
Selecting a CT perfusion protocol should be based on the patient's risk profile. In low-risk patients, performing CCTA first is recommended. It then may be followed by CTP if coronary stenosis is suspected. In high-risk patients such as those with known coronary artery disease, performing stress CTP first would be beneficial due to enhanced sensitivity for detection of ischemia, which is sometimes more important than morphology of coronary artery in clinical decision-making.
To obtain optimal CTP images, high-end CT scanners with high temporal resolution, wide z-axis coverage, and algorithms to reduce artifacts such as beam hardening are required. Even with the technological innovations of CT scanners and dose reduction software, a major inhibitor of using the technology is the need for two scans, which increases radiation exposure with an additional contrast load. Still, there is growing interest in the technology, and research is being undertaken throughout the world.
Kitagawa and colleagues have been also working on methods to improve the clinical utility of CTDE, which is generally limited due to poor contrast-to-noise ratio and artifacts. Their use of targeted spatial frequency filtration (TSFF) in a study of 40 patients who underwent comprehensive cardiac CT showed that TSFF with image averaging can significantly improve image quality of CTDE and considerably enhance interobserver reproducibility of infarct sizing.
Looking at the bigger picture, CCTA remains the noninvasive reference standard to efficiently assess obstructive coronary artery disease and the status of coronary vasculature. It has high sensitivity and negative predictive value in its ability to assess coronary artery anatomy and provide direct visualization of atherosclerotic plaque compared with invasive coronary angiography. However, CCTA has limited ability to determine physiologic and hemodynamic significance of coronary artery disease. When indeterminate coronary stenosis is identified, functional imaging modalities such as stress cardiac MRI, single-photon emission CT, and stress echocardiography are used to detect myocardial ischemia.
FFR, on the other hand, is the gold standard for determining lesion-specific ischemia. It is an invasive, expensive, and time-consuming procedure that is performed when a patient is undergoing invasive coronary angiography (ICA). It assesses blood flow and identifies lesions that need to be revascularized. Catheterization is performed using a pressure wire with a sensor on its tip that measures actual blood flow through a coronary artery, identifies lesions, and can help determine lesion severity.
Also in today's session, Dr. John Hoe of Mount Elizabeth Medical Center in Singapore, discussed another emerging technology: plaque imaging with CCTA. The presenters also looked into the future and speculated about which of these techniques will change clinical practice.
Originally published in ECR Today on 7 March 2015.
Copyright © 2015 European Society of Radiology



















