VIENNA - Breast MRI already has high sensitivity, but can it be even higher? The answer is yes, if computer-aided detection (CAD) is thrown into the mix, according to a presentation at ECR 2015. In fact, the CAD system detected previously missed cancers nearly as well as it did screen-detected cancers.
"If one just looks at the values for sensitivity, it seems that no one can miss anything in breast MRI. But is that true?" asked Albert Gubern Mérida, a PhD candidate at the Diagnostic Image Analysis Group of Radboud University Nijmegen Medical Center in the Netherlands. According to recent studies, it still doesn't seem to be the case, as it was found that around 50% of these cancers could have been detected earlier.
Using CAD for suspected abnormalities in MRI may prevent reading errors in breast cancer screening of women at high risk, he said. Gubern Mérida and colleagues evaluated the performance of a CAD system in detecting breast cancers missed in screening, comparing it with how well the system performed for screen-detected cancers.
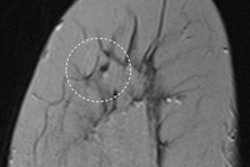
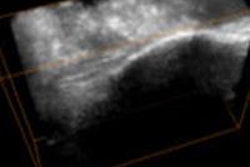
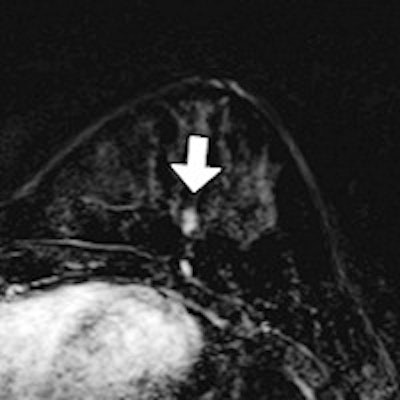
 Breast cancer lesions that were missed in screening with MRI but detected by CAD. The arrows indicate the lesions. All images courtesy of Albert Gubern Mérida, PhD.
Breast cancer lesions that were missed in screening with MRI but detected by CAD. The arrows indicate the lesions. All images courtesy of Albert Gubern Mérida, PhD.Dynamic, contrast-enhanced (DCE)-MRI studies were collected from 163 women participating in a high-risk screening program. The data included 26 scans with screen-detected cancers and 23 scans with cancers that were initially missed.
Among the 23 scans, 10 cancers were retrospectively visible (BI-RADS 4/5) and 13 cancers were minimally visible (BI-RADS 2/3) in prior MRI screening exams but were reported normal. The cancers were detected at the following screening round. Also, 114 normal scans with no sign of breast cancer were included in the study. Lesions were annotated on the first postcontrast subtraction image.
The CAD system, which was developed in-house, was evaluated using free-response receiver operator characteristics (FROC) analysis and bootstrapping. A CAD finding was considered a true positive when its center was inside a lesion annotation, Gubern Mérida said. The false-positive rate was determined on the normal cases.
At four false positives per case, the sensitivity for screen-detected lesions was 0.80. For lesions that were visible or minimally visible in prior false-negative studies, the sensitivities were 0.69 and 0.47, respectively.
"To conclude, we show that the CAD system is able to detect lesions that were missed with screening MRI, with almost as high sensitivity as screen-detected cancers," Gubern Mérida said. "The clinical relevance is that the introduction of such a system can really help ... to avoid these errors."
The CAD system can be improved, however. The researchers plan to study possible ways of integrating CAD in clinical practice.
"For instance, we think it can be useful to facilitate more efficient analysis of 4D data by automatically displaying the most suspicious slices and time points based on the automatically detected CAD markers," he wrote in an email to AuntMinnieEurope.com. "In this way, some seconds of scrolling and looking for the lesion can be saved, which is quite relevant in screening settings."
They are also investigating the application of advanced image processing or visualization techniques on areas marked by CAD to artificially enhance certain regions in the image without directly pointing to them. In breast DCE-MRI, such techniques can be applied to maximum intensity projection (MIP) images, in particular.
"For example, in a MIP, a lesion that is obscured by prominent background enhancement but is detected by the CAD on the 3D space could be artificially enhanced and therefore be visible in the MIP image," he wrote.