VIENNA - A new integrated circuit (IC) CT detector may improve the ability of clinicians to accurately grade coronary artery stenoses visualized during coronary CT angiography (CCTA), especially when combined with thin-slice imaging and iterative reconstruction, researchers reported on Sunday at ECR 2013.
In a study that incorporated both phantom and clinical images, the IC detector -- applied with and without iterative reconstruction -- showed significantly improved image quality, concluded the group from University Hospital Zurich in Switzerland.
"Our study suggests that the grading of stenosis in coronary CT angiography is improved by using an integrated circuit combined with iterative reconstruction and a 0.5-mm slice thickness," said Dr. Fabian Morsbach, a first-year resident in the hospital's department of diagnostic and interventional radiology.
Current conventional CT scanners are equipped with detectors built in a discrete circuit (DC), which means that the diodes send out their analog signals to an analog-to-digital converter (ADC) circuit board, then onto a separate digital circuit board, introducing signal noise along the way that makes its way into images, Morsbach explained. But a new generation of detectors combines the photodiodes and the ADCs on a single board into an IC detector.
"This means that the path that the analog signal has to take is significantly reduced with the ADCs on the same board; this results in decreased electronic noise, which can be used to reconstruct images with reduced slice thickness when combined with iterative reconstruction," he said. "What we wanted to do was assess the value of an integrated detector, which potentially improves the spatial resolution in coronary CT angiography regarding image quality and stenosis quantification when compared to a conventional detector."
The study included both a phantom arm that quantified image quality in the new (IC) and conventional (DC) detector with and without the use of iterative reconstruction and also a patient study that looked at image quality with the use of both iterative reconstruction and FBP but only on the new detector -- allowing the research team to clearly distinguish the effects of each technology in at least the phantom portion of the study.
All images were acquired with 128-section dual-source CT system equipped with IC (Stellar, Siemens Healthcare) and for the phantom arm conventional detector technology as well. The custom-made cardiac phantom was equipped with seven tubes that incorporated different kinds of stenoses ranging from fatty to heavily calcified plaques, with a range of 10% to 90% for each tube and each plaque type, Morsbach said. It was scanned at 0°, 45°, and 90° orientations to the z-axis of the CT scanner table.
Phantom data were reconstructed using filtered back projection with a slice thickness of 0.6 mm and iterative reconstruction at the same slice thickness. For data acquired with the integrated detector, images were reconstructed with iterative reconstruction and a slice thickness of 0.5 mm. The phantom images were analyzed for image quality and stenosis degree.
After the phantom study, the group examined 30 patients (11 women, mean age 62 ± 13 years; mean heart rate 81 ± 17 bpm) undergoing CCTA on the scanner with the IC detector, reconstructed with both FBP and iterative reconstruction. The images were analyzed for image quality and stenosis degree.
Better in phantoms and humans
Results showed that image quality was significantly higher for images acquired with the IC detector as compared with the conventional detector. In addition, image noise was significantly reduced for the IC detector compared with the conventional detector when applying iterative reconstruction.
"Image noise is lower for filtered back projection but not significantly so, and when you compare iterative reconstruction with the conventional detector and the integrated detector, you find a significant decrease in noise just by having the new detector," Morsbach said. "When we reconstructed thinner slices for iterative reconstruction, we saw a slight increase in noise but not significantly so."
More important, the integrated detector yielded significantly more accurate results for stenosis quantification compared with the conventional detector, both for filtered back projection and iterative reconstruction, both for 5-mm and 6-mm reconstructions, Mosbach said. So the use of iterative reconstruction with a slice thickness of 0.5 mm obtained by the IC detector significantly improved accuracy in the phantom compared with filtered back projection. Improvements were found using the IC detector for all rotational angles, but especially for images acquired at a 90° angle.
"The differences were apparent at all projectional angles but were most pronounced at the 90° angle, where we see a slight decrease in measurement error for the integrated detector," Morsbach said.
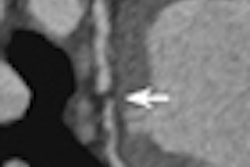
 Phantom coronary CT angiography images with a slice thickness of 0.5 mm reconstructed with iterative reconstruction obtained by the integrated circuit detector improved measurement accuracy by the greatest degree. A 60% stenosis at filtered back projection appears to occupy the entire lumen, with the conventional detector, while demonstrating nonstenosed lumen using the new detector and even more with the addition of iterative reconstruction. All images courtesy of Dr. Fabian Morsbach.
Phantom coronary CT angiography images with a slice thickness of 0.5 mm reconstructed with iterative reconstruction obtained by the integrated circuit detector improved measurement accuracy by the greatest degree. A 60% stenosis at filtered back projection appears to occupy the entire lumen, with the conventional detector, while demonstrating nonstenosed lumen using the new detector and even more with the addition of iterative reconstruction. All images courtesy of Dr. Fabian Morsbach.The patient arm also showed significantly (p < 0.001) higher image quality -- and stenoses were quantified as significantly smaller using iterative reconstruction: 47.6% versus 42.1% (mean difference 5.5%, p = 0.009).
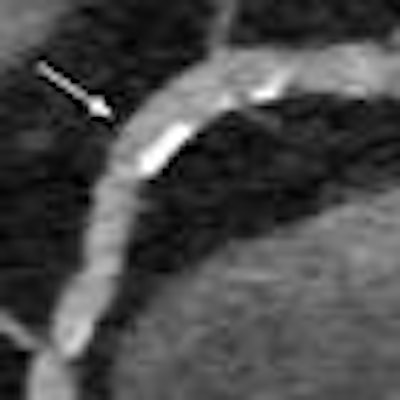
 Use of the IC detector in coronary CT angiography yielded higher image quality in patients, both with (right) and without (left) the use of iterative reconstruction.
Use of the IC detector in coronary CT angiography yielded higher image quality in patients, both with (right) and without (left) the use of iterative reconstruction."With filtered back projection and the conventional detector at the 60% stenosis, it seems like it almost no lumen left, but when you go to the integrated detector you can see the effect, which becomes really apparent when you look at the combination of the thinner slice thickness, iterative reconstruction, and the new detector, where you can still discern the lumen at 60% stenosis," he said, and the difference is also visibly apparent at the 50% stenosis level.
As for limitations, the phantom did not mimic cardiac movement, he said, and the patient study was limited to IC but not DC scans. Finally, there was no angiographic reference standard to which the results could be compared.
Still, the results suggest that accuracy for grading of stenosis severity in CCTA is improved using an integrated detector, especially when combined with iterative reconstruction and 0.5-mm slice thickness, he said. The improvement in stenosis grading in the patient arm may be largely attributable to the use of iterative reconstruction, which has been shown to reduce blooming artifacts, Mosbach said in response to a question from session moderator Dr. Gudrun Feuchtner, PhD, from Innsbruck Medical University in Austria.