One of Europe's leading exponents of CT colonography (CTC) has called for much greater harmonization and drastically improved funding for the reimbursement of this emerging procedure.
"Reimbursement is a key factor for the development not only of CTC but also of any imaging method," said Dr. Andrea Laghi of the department of radiological sciences (Polo Pontino) at the University "La Sapienza" in Latina, Italy. "Considering the current economic situation, getting reimbursement for a new technique is much more difficult than in the past, especially if there are strongly competing alternatives."
Major differences in reimbursement currently exist across Europe, and even within individual countries, as in the case of Italy and Austria. The overall situation is poor, and strong efforts need to be made in the near future to try to solve the difficulties, he explained. In general, CTC is not reimbursed for screening in any European country, with the recent exception of Spain, where a private insurer decided to cover colorectal cancer screening with CTC. In some regions of the U.K. and Italy, it forms part of official screening programs offered to fecal occult blood test (FOBT)-positive patients with an incomplete colonoscopy, but this is not the norm, he added.
"Cost is one of the leading factors for both public healthcare systems and private insurers. Misinformation and turf battles with other specialists are additional reasons, together with the heterogeneity of the results reported in the literature. Finally, standards and training are having an impact," stated Laghi, a speaker about the topic at Friday's ECR 2011 State of the Art Symposium. "CTC needs to be reimbursed as a standard CT examination. This is what happens in the Netherlands, and in some Italian regions. It will cost money, but at least a program can be started."

 Left: Coronal reformatted view showing a pedunculated polyp of the sigmoid colon. Right: Volume-rendered endoluminal view of the same pedunculated polyp. In both images, the curved arrow indicates the stalk, and the straight arrow indicates the head of the polyp. Images courtesy of Andrea Laghi, MD.
Left: Coronal reformatted view showing a pedunculated polyp of the sigmoid colon. Right: Volume-rendered endoluminal view of the same pedunculated polyp. In both images, the curved arrow indicates the stalk, and the straight arrow indicates the head of the polyp. Images courtesy of Andrea Laghi, MD.As an examination designed for polyp and tumor detection in the colon, CTC has now reached a sufficient level of competency, making the double-contrast barium enema an obsolete examination in 2011, according to fellow ECR presenter Dr. Philippe Lefere, a radiologist at Stedelijk Ziekenhuis in Roeselare, Belgium. As the implementation of CTC moves ahead, general radiologists must become aware this technique can play a significant role by scrutinizing both symptomatic and asymptomatic patients for polypoid and tumoral lesions in the colon.
In recent multicenter trials, CTC showed very good results of polyp detection, and its accuracy approaches that of optical colonoscopy, he pointed out. CTC is now an indication for patients after an incomplete optical colonoscopy, patients with a contraindication to optical colonoscopy, and patients unwilling to undergo optical colonoscopy. CTC is a reliable tool for colorectal cancer screening in the patient at average risk for colorectal cancer.

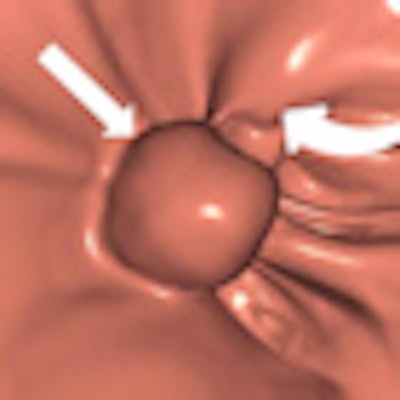
 Left: Large pedunculated polyp in the sigmoid (white arrow). Right: Corresponding 3D image of this pedunculated polyp with a 2-cm head (white arrow). Images courtesy of Philippe Lefere, MD.
Left: Large pedunculated polyp in the sigmoid (white arrow). Right: Corresponding 3D image of this pedunculated polyp with a 2-cm head (white arrow). Images courtesy of Philippe Lefere, MD.Moreover, the procedure is patient-friendly and it can be performed on an outpatient basis. No sedation is necessary, the examination time is short, it can be performed the same day as the optical colonoscopy, it can detect important pathology outside of the colon, and patient preparation is possible without interruption of normal daily activities, Lefere said. The main drawbacks are that radiation is used, polypectomy is not possible, there is the potential for superfluous explorations (iatrogenic pathology), patient preparation is still needed, it involves a relatively steep learning curve, and long interpretation times during the initial phase.
"Technical advances with the introduction of the latest multislice scanners, and improvements in x-ray tubes with the use of tube current modulation, and beam-shaping filters have decreased radiation dose," he stated. "Further improvements of CT scanners together with iterative reconstruction techniques will allow more decreases in the radiation dose in general. This will bring radiation doses for CTC to a negligible level."
The use of (ultra)low dose in CTC is possible because of the high contrast between the luminal gas and the colonic structures. A low dose of 120 kV and 50 mAs is recommended for CTC in asymptomatic patients. Taking into account this low dose, the good performance of CTC, the prevalence of colorectal adenomas, and/or cancer, and the patient's age (usually more than 50 years old), there is a clear benefit of CTC versus no screening, with a very low risk of radiation-induced cancer (0.05%), Lefere noted.

 Left: Small 7-mm polyp in colon, drowned in tagged fluid in supine position (white arrow). Right: Corresponding 3D view in prone position shows the same polyp (white arrow). Images courtesy of Philippe Lefere, MD.
Left: Small 7-mm polyp in colon, drowned in tagged fluid in supine position (white arrow). Right: Corresponding 3D view in prone position shows the same polyp (white arrow). Images courtesy of Philippe Lefere, MD.Using a low dose may cause excess image noise, resulting in pseudoenhancement, but this problem can be solved by comparing the lesion with a tagged stool elsewhere in the colon, or by smoothing the abdominal window. When starting CTC as a novice, a dose of 80 mAs should be used to avoid image noise, he advised.
Along with his colleague Dr. Stefaan Gryspeerdt, Lefere has addressed CTC's potential pitfalls in a comprehensive paper published online January 4 in Insights into Imaging. Their top tips are to perform state-of-the-art CTC (preparation based on fecal tagging, along with colonic distension with CO2 plus injector, dual positioning, and smooth muscle relaxation), remember the general principles of interpretation, and take special care when examining the rectum and caecum.
It is important to make CTC a really efficient tool for polyp detection performed reliably by a large community of radiologists, and to confirm the good results obtained in trials. Structured education with ongoing quality assurance (QA) will need to be implemented, Lefere stated. Recommendations for CTC education need to be further elaborated, and a lot of work is being done in this area by the European Society of Gastrointestinal and Abdominal Radiology's CTC committee. Developing good collaboration with gastroenterologists is another vital task because this will enable QA through the establishment of patient guidelines and follow-up of patients with a lesion detected by CTC.
"The future is mainly in the hands of radiologists active in this field," Laghi predicted. "We need vendors to provide us with the right tools. We should continue working to improve on the procedure from a technical point of view, with more comfortable bowel preparation, minimization of radiation exposure, and faster and more accurate reading, possibly with the help of computer-aided diagnosis software. But we should also pursue other goals, including the development of a QA program, strong governance, plus audit, and training."
Originally published in ECR Today March 4, 2011.
Copyright © 2011 European Society of Radiology



















