VIENNA - Single-beat scanning not only enables significant radiation dose reductions in coronary CT angiography (CTA), the short duration of the scan permits drastically lower contrast doses as well, at least in patients with regular heartbeats and no arrhythmias.
In comparison, coronary CTA on 64-slice scanners requires a scan duration of approximately 14 seconds to acquire the heart volume over seven to eight beats, with a corresponding iodinated contrast dose of 100-200 mL.
Single-beat coronary CTA with 320-slice CT acquires the heart volume in approximately one second with about half of the contrast dose. But even that level is higher than necessary, said Dr. Alexander Lembcke from Charité Medical University in Berlin.
For 320-detector-row coronary CTA, "the standard contrast media injection protocol recommended by the manufacturer is 70 mL at an injection rate of 5 mm/sec, so there's a large discrepancy between the duration of the contrast injection at 40 seconds and the duration required to obtain the entire volume of the heart in one second or less," Lembcke said in a presentation Friday at the European Congress of Radiology (ECR).
The investigators sought to design a low-dose acquisition protocol that also minimized the contrast dose.
They scanned 24 patients (16 men, eight women; ages 36-74 years) who were referred for coronary CTA. The cohort had a mean body mass index (BMI) of 21.9 (range, 18-26) and heart rate ranging from 54 to 69 bpm, and all patients were in sinus rhythm.
Patients were excluded if their heart rate after the administration of beta-blockers was higher than 65 bpm -- or weight was higher than 85 kg, left ventricular function was less than 40% at echocardiography, or if there were contraindications to iodinated contrast media.
The patients were scanned using 320-detector-row CT (AquilionOne, Toshiba, Otawara, Japan) at 100 kV, 300-450 mA, 0.5-mm collimation with a 0.25 reconstruction increment, and 350 msec rotation time.
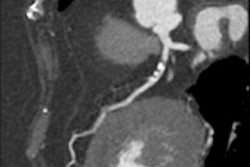
A single-beat acquisition with prospective electrocardiogram triggering at 75% of the RR interval was performed following intravenous administration of 35 mL of a concentrated contrast medium (Ultravist, Bayer HealthCare Pharmaceuticals, Wayne, NJ) at 7.5 mL/sec, followed by a saline chaser at the same flow rate.
"The actual acquisition window was 400 to 500 msec to compensate for any slight changes of the heart rhythm," Lembcke said. Scanning was started using bolus tracking when opacification of a region of interest in the left ventricle reached 300 HU.
Vessel attenuation, image noise, and contrast-to-noise ratio were measured, and overall image quality and diagnostic confidence were rated for each patient.
All scans were of diagnostic quality, and attenuation values measured by density in the aortic root ranged from 312 to 523 HU, and image noise ranged from 38 to 56 HU, with a contrast-to-noise ratio of 7.8 to 16.3 HU.
"We had no stairstep artifacts; only mild or no motion artifacts were observed," he said. All datasets were rated as having good (n = 14) or excellent image quality (n = 10), and diagnostic confidence was rated high (n = 11) or very high (n = 13) in all patients.
The calculated radiation dose based on the dose-length-product displayed on the scanner console ranged between 1.3 and 2.2 mSv.
"In selected patients -- and I would like to emphasize 'selected patients' -- prospectively triggered gated 320-slice coronary CTA using a wide-area detector CT offers the possibility of dramatically reducing radiation exposure and, at the same time, reducing the amount of contrast material needed," Lembcke concluded.
Session moderator Dr. Dominik Fleischmann from Stanford University in Stanford, CA, asked at what point the results would be inadequate for larger patients, noting that contrast volume might be insufficient to achieve adequate opacification, and the signal-to-noise ratio would be reduced as well.
The protocol appears to work well for any patient less than 85 kg with normal sinus rhythm and normal left ventricular function, Lembcke said. Even those with higher heart rates who require a longer scan time (more than two heartbeats at 320-slice CTA) should be able to use the protocol, he added, because opacification with 35 mL of contrast remains high for the one or two heartbeats following the target heartbeat.
By Eric Barnes
AuntMinnie.com staff writer
March 6, 2009
Related Reading
Opacification at 320-detector-row CT distinguish normal, stenosed vessels, March 6, 2009
320-detector-row CT cuts dose in triple rule-out exams, February 12, 2009
Flexibility of 320-slice CT boosts cardiac imaging options, October 3, 2008
Prospective gating minimizes dose in 320-slice CTA, August 5, 2008
Fourth-generation MDCT scanners do cardiac differently, July 8, 2008
Copyright © 2009 AuntMinnie.com