A prizewinning study has highlighted that in the proper hands, ultrasound is a valuable diagnostic tool that can accurately assess pathologies of the fingernails and toenails, including subungual melanoma.
Nail disorders found in daily clinical practice tend to be diagnosed on the basis of clinical findings, but imaging may be needed for a better evaluation. That was the main message of new research by Dr. Carolina Avila de Almeida and colleagues from the National Institute of Cancer (INCA) and Alta Excelência Diagnóstica, Rio de Janeiro, Brazil.
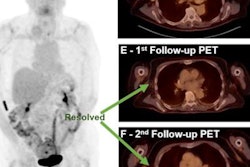
 65-year-old woman reported nail dystrophy for several months. Top ultrasound image shows cortical bone rupture (yellow arrows), and Power Doppler identified hypervascularization. The diagnosis was nail melanoma Clark Level 3, where the melanoma cells are touching the next layer down, known as the reticular dermis, or deep dermis. All figures courtesy of Drs. Carolina Avila de Almeida and Clarissa Canella and RSNA.
65-year-old woman reported nail dystrophy for several months. Top ultrasound image shows cortical bone rupture (yellow arrows), and Power Doppler identified hypervascularization. The diagnosis was nail melanoma Clark Level 3, where the melanoma cells are touching the next layer down, known as the reticular dermis, or deep dermis. All figures courtesy of Drs. Carolina Avila de Almeida and Clarissa Canella and RSNA."Longitudinal melanonychia on the ungual plate is a common clinical finding, and it has been established that repetitive trauma is a risk factor for melanoma," they noted in an RSNA 2021 e-poster that received a magna cum laude award.
In such cases, radiologists must look for a well-defined hypoechoic area with increased thickness and decreased echogenicity of the nail bed, which frequently erodes into the bone margin of the distal phalanx and nail plate, the authors explained.
Other tumor and tumor like-lesions
In addition to melanoma, it is important to keep in mind the following pathologies:
- Cysts. These are solitary, clear, or flesh-colored nodules that develop on the dorsal digits between the distal and interphalangeal (IP) joint and the proximal nail fold. They may be associated with degenerative changes in the distal IP joint, or not. The key points include anechoic appearance (may contain echogenic foci when content is more viscous), no vascularization, and communication with IP joint.
- Squamous cell carcinoma. This rare malignant tumor originates underneath the nail plate and grows slowly. A strong association with different conditions (e.g. trauma, radiation exposure, high-risk human papillomavirus) has been reported. These tumors may result from an ill-defined injury, and are heterogeneous and hypoechoic on ultrasound, appearing hypervascularized, with erosion of the nail plates and distal phalynx.
- Exostosis. Subungual exostosis is a common benign bone tumor that occurs in the distal phalanges and can be a source of pain and nail deformity. Look out for a hyperechogenic subungual sonographic image that continues with the bone surface of the phalanx.
- Fibroma. Periungual fibromas are rare benign tumors that may be acquired or associated with tuberous sclerosis. Periungual fibroids may place excessive pressure on the nail matrix, resulting in nail dystrophy and pain. Fibromas are located in the proximal nail fold and are eccentric, which may affect the nail matrix concomitantly (dumb-bell appearance).
- Neuroma. Neuromas are tumors of benign neural origin. They are located in the periungual region and most of the lateral and medial folds, where the nerves in the fingers and toes are found. Clinical signs include onychodystrophy and longitudinal grooves. Key points: periungual location, eccentric, related to the lateral nail fold, and well-defined.
- Lipoma. Lipomas are one of the most common benign soft tissue tumors. They are rarely found on the fingers. Most cases are painless and are characterized by well-defined and circumscribed lesions, hyperechoic, oval, with little or no vascularization.


Also, a glomus tumor is a rare benign tumor originating from the neuromyoarterial glomus body (arteriovenous anastomosis) responsible for thermoregulation. Most of these tumors occur in the hands. The classic triad of symptoms is localized tenderness, severe pain, and cold sensitivity. Watch for a hyperechogenic subungual sonographic image that continues with the bone surface of the phalanx, the authors recommended.
In addition, onychomatricoma is a rare benign fibroepithelial tumor of the nail matrix. The tumor affects mainly women in the fifth decade of life, and it is typically slow-growing and painless. Key points: hyperechoic band-like appearance with hyperechoic lines, eccentric location, hypovascular, no bone remodeling, and thickening of plaques.
Technique and equipment
Use a lot of cold gel on the nail surface and as little pressure as possible, resting your hand on the examination table, the authors advised. Choose the correct transducer (>15 MHz), keep the focus on the nail surface, try to visualize the entire nail, and use power Doppler and Superb microvascular imaging (SMI) or microvascular flow imaging (MVI/MV-flow).
Higher frequency leads to lower penetration but higher resolution (18 MHz offers better visualization of the nail unit; 33 MHz gives better visualization of the nail plates). The focus should be placed superficially on the target of interest. Power Doppler offers a speed slower than 5 cm/s and can remove the artifact, they continued.
Among the factors to consider are the thickness of the nail bed, the distal phalanx (integrity or remodeling of cortex), and the nail plate (thickness, convexity, and trilaminar pattern). Look for space-occupying injuries and always check the vascularization of the nail apparatus, the authors concluded.