A COVID-19-specific CT reporting system called CO-RADS can help clinicians quickly diagnose the disease when patients present in the emergency department, according to a study published on 17 November in Radiology.
The results further confirm CT's role in coping with the COVID-19 crisis, wrote a team led by Dr. Steven Schalekamp, PhD, of Radboud University Medical Center in Nijmegen, the Netherlands.
"During this pandemic we demonstrated high performance of chest CT using the COVID-19 reporting and data system (CO-RADS) for the diagnosis of COVID-19 in clinical practice," the group wrote. "This ... suggests that chest CT can be used to optimize/expedite emergency care for patients suspected of having COVID-19 pneumonia."
Since the COVID-19 pandemic began, clinicians have been seeking fast and reliable ways to diagnose the disease. Reverse transcription polymerase chain reaction (RT-PCR) testing is considered the gold standard, but it does have drawbacks, including limited sensitivity and time needed for results, the group noted. CT offers the benefit of fast results, but its use has been debated.
Schalekamp's team sought to evaluate the efficacy of using the CO-RADS system for chest CT in patients with moderate to severe symptoms of COVID-19. The system scores pulmonary involvement using a scale of 1 to 5 (1 = normal, 5 = typical for COVID-19). A score of 4 or higher is considered highly indicative of COVID-19.
 Example chest CT scans of a patient with a true-positive CO-RADS 4 score. (a,b) Two axial slices and (c) a coronal slice of a 79-year-old female with nine days of symptoms. CT shows diffuse ground-glass opacities close to visceral pleural surfaces but superimposed on emphysematous changes. Also note the widened esophagus. COVID-19 was RT-PCR confirmed. Images courtesy of the RSNA.
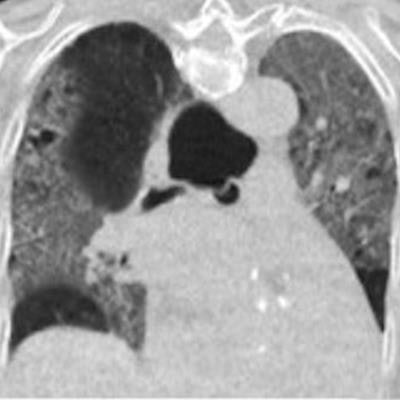
Example chest CT scans of a patient with a true-positive CO-RADS 4 score. (a,b) Two axial slices and (c) a coronal slice of a 79-year-old female with nine days of symptoms. CT shows diffuse ground-glass opacities close to visceral pleural surfaces but superimposed on emphysematous changes. Also note the widened esophagus. COVID-19 was RT-PCR confirmed. Images courtesy of the RSNA. Example chest CT scans of a patient with a false-positive CO-RADS 4 score. (d, e) Two axial slices and (f) a coronal slice of a 51-year-old female with two days of symptoms. CT shows bilateral multifocal areas of consolidation with halo and subtle areas of ground glass without contact to visceral pleural surfaces. RT-PCR for SARS-CoV2 was repeatedly negative and an alternative diagnosis was established with a blood culture-confirmed line sepsis. Images and caption courtesy of the RSNA.
Example chest CT scans of a patient with a false-positive CO-RADS 4 score. (d, e) Two axial slices and (f) a coronal slice of a 51-year-old female with two days of symptoms. CT shows bilateral multifocal areas of consolidation with halo and subtle areas of ground glass without contact to visceral pleural surfaces. RT-PCR for SARS-CoV2 was repeatedly negative and an alternative diagnosis was established with a blood culture-confirmed line sepsis. Images and caption courtesy of the RSNA.The study included 1,070 patients who presented in the emergency departments of six Dutch medical centers between March and April. Chest CT exams were scored using CO-RADS and the scores compared with RT-PCR results and a clinical reference standard that included factors such as COVID-19 contact history, oxygen therapy, and the timing of RT-PCR testing. The investigators rated CT's performance using receiver operating characteristics curve (AUC) analysis and odds ratios; they also considered the timing of patients' symptoms (from less than 48 hours to more than seven days).
The CO-RADS system showed comparable diagnostic performance to RT-PCR testing and the clinical reference standard, especially after patients had symptoms for 48 hours or more.
| Performance of CO-RADS for diagnosing COVID-19 | ||||
| RT-PCR reference standard | Clinical reference standard | CO-RADS at positivity threshold of ≥ 4 using RT-PCR as reference standard | CO-RADS at positivity threshold of ≥ 4 using clinical reference standard | |
| AUC | 0.87 | 0.87 | 0.87 | -- |
| Sensitivity | -- | -- | 86% | 77% |
| Specificity | -- | -- | 81% | 90% |
| Odds ratio of COVID-19 diagnosis | -- | -- | 25.9 | 30.6 |
Although the study results were positive, clinicians must keep in mind that CT's role in COVID-19 diagnosis continues to evolve, Dr. Brett Elicker of the University of California, San Francisco wrote in an accompanying editorial.
"While CT is helpful in the detection and characterization of alternative causes of pulmonary symptoms ... its role directly related to COVID-19 infection itself still has yet to be determined," Elicker wrote. "The results of this study, however, can form a foundation for other investigations whose goal is to further elucidate the potential roles of CT in the detection and characterization of this deadly disease."